

Vitamin D deficiency and the risk of tuberculosis: a meta-analysis
- PMID: 28096657
- PMCID: PMC5207333
- DOI: 10.2147/DDDT.S79870
Vitamin D deficiency and the risk of tuberculosis: a meta-analysis
Abstract
Background and aim: To conduct meta-analyses of all published studies on various aspects of association between vitamin D and tuberculosis (TB).
Methods: PubMed and Web of Knowledge were searched for all properly controlled studies on vitamin D and TB. Pooled odds ratio, mean difference or standardized mean difference, and its corresponding 95% confidence interval were calculated with the Cochrane Review Manager 5.3.
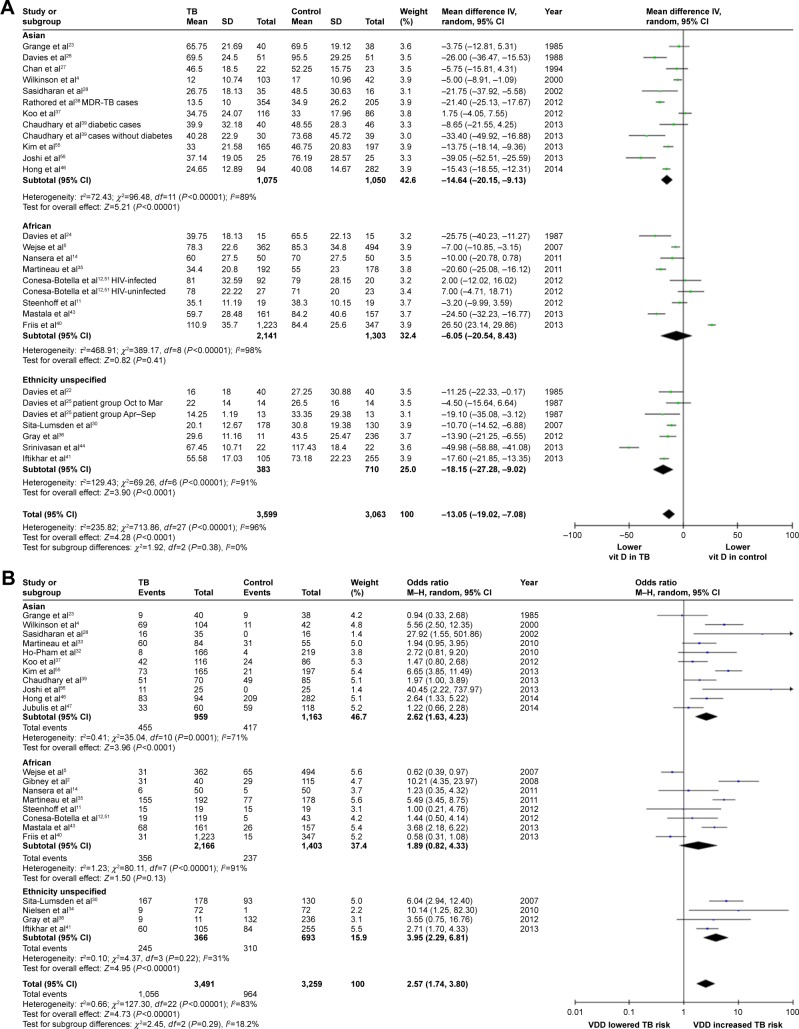
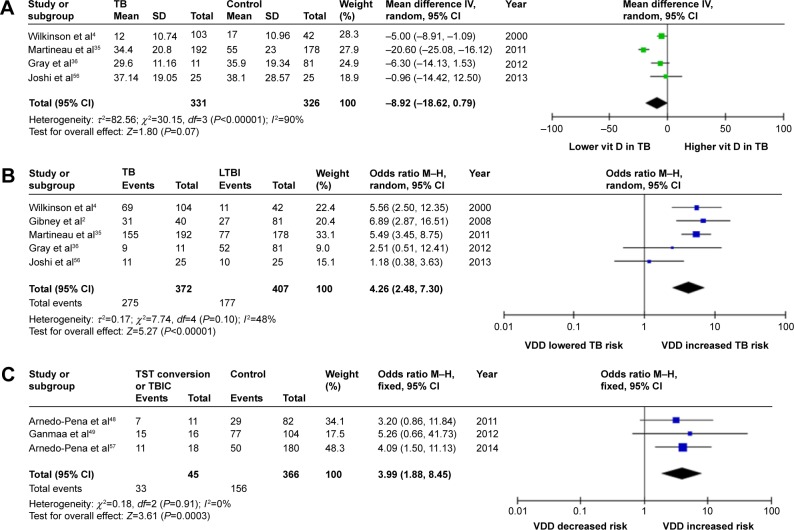
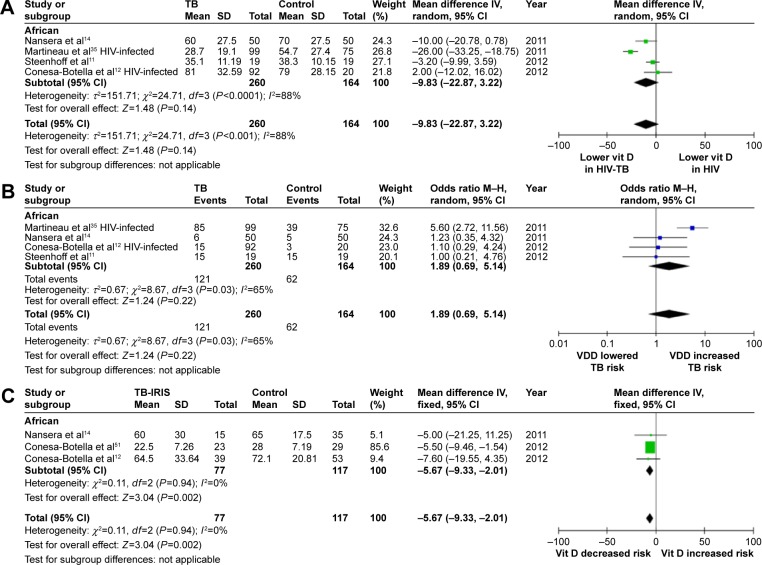
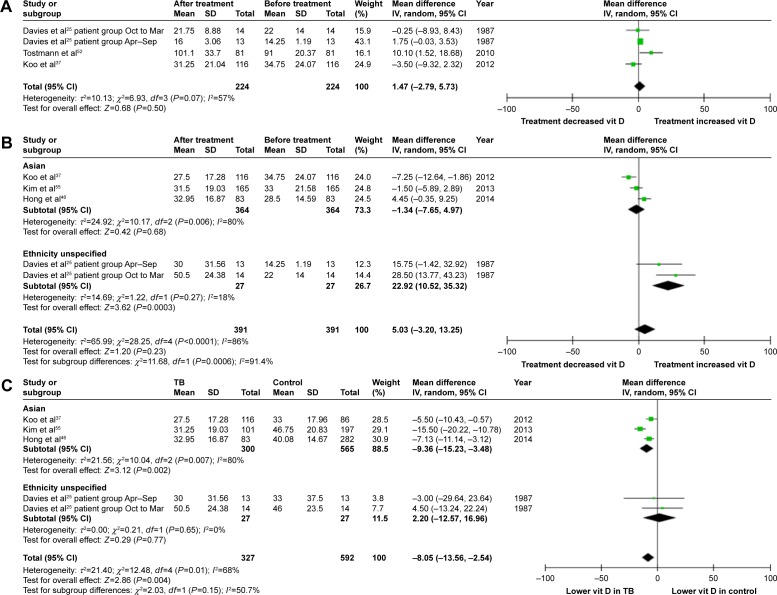
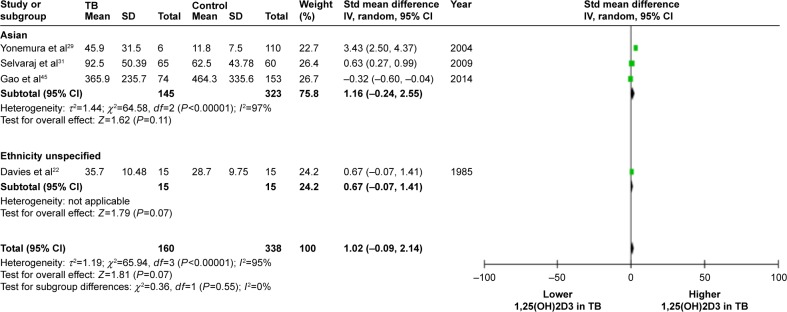
Results: A significantly lower vitamin D level was found in TB patients vs controls; vitamin D deficiency (VDD) was associated with an increased risk of TB, although such an association was lacking in the African population and in the human immunodeficiency virus-infected African population. A significantly lower vitamin D level was found in human immunodeficiency virus-TB-coinfected African patients receiving antiretroviral treatment who developed TB-associated immune reconstitution inflammatory syndrome vs those who did not develop TB-associated immune reconstitution inflammatory syndrome. VDD was associated with an increased risk of developing active TB in those subjects with latent TB infection and with an increased risk of tuberculin skin test conversion/TB infection conversion, and the trend toward a lower vitamin D level in active TB patients vs latent TB infection subjects did not reach statistical significance, indicating that VDD was more likely a risk factor than a consequence of TB. This concept was further strengthened by our result that anti-TB treatment did not affect vitamin D level in TB patients receiving the treatment.
Conclusion: Our analyses revealed an association between vitamin D and TB. VDD is more likely a risk factor for TB than its consequence. More studies are needed to determine whether vitamin D supplementation is beneficial to TB prevention and treatment.
Keywords: 25-hydroxyvitamin D; meta-analysis; tuberculosis; vitamin D; vitamin D deficiency.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Comment in
-
Vitamin D deficiency and tuberculosis: what about body mass index?Drug Des Devel Ther. 2017 Apr 11;11:1193-1194. doi: 10.2147/DDDT.S133094. eCollection 2017. Drug Des Devel Ther. 2017. PMID: 28442893 Free PMC article. No abstract available.
References
-
- Kim JH, Park JS, Cho YJ, et al. Low serum 25-hydroxyvitamin D level: an independent risk factor for tuberculosis? Clin Nutr. 2014;33(6):1081–1086. - PubMed
-
- Gibney KB, MacGregor L, Leder K, et al. Vitamin D deficiencyis associated with tuberculosis and latent tuberculosis infection in immigrants from sub-Saharan Africa. Clin Infect Dis. 2008;46(3):443–446. - PubMed
-
- Chocano-Bedoya P, Ronnenberg AG. Vitamin D and tuberculosis. Nutr Rev. 2009;67(5):289–293. - PubMed
-
- Wilkinson RJ, Llewelyn M, Toossi Z, et al. Influence of vitamin D deficiency and vitamin D receptor polymorphisms on tuberculosis among Gujarati Asians in West London: a case-control study. Lancet. 2000;355(9204):618–621. - PubMed
-
- Wejse C, Olesen R, Rabna P, et al. Serum 25-hydroxyvitamin D in a West African population of tuberculosis patients and unmatched healthy controls. Am J Clin Nutr. 2007;86(5):1376–1383. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
