

Diffuse Large B-Cell Lymphoma in the Era of Precision Oncology: How Imaging Is Helpful
- PMID: 28096718
- PMCID: PMC5240489
- DOI: 10.3348/kjr.2017.18.1.54
Diffuse Large B-Cell Lymphoma in the Era of Precision Oncology: How Imaging Is Helpful
Abstract
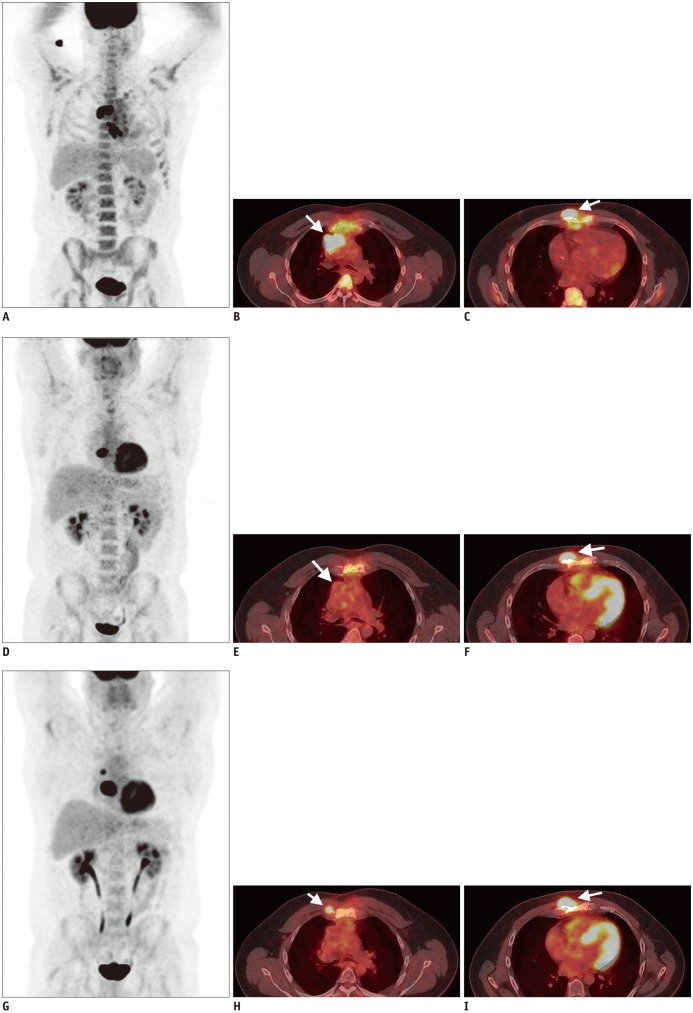
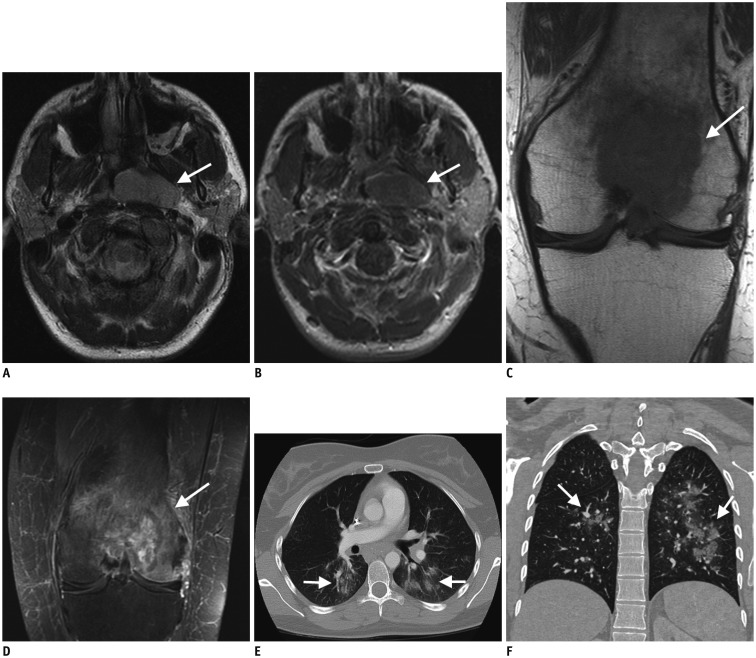
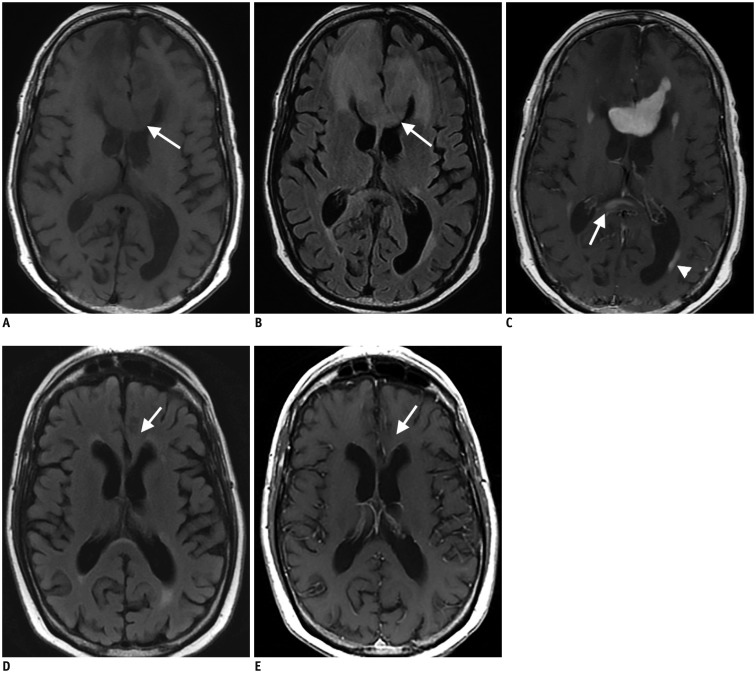
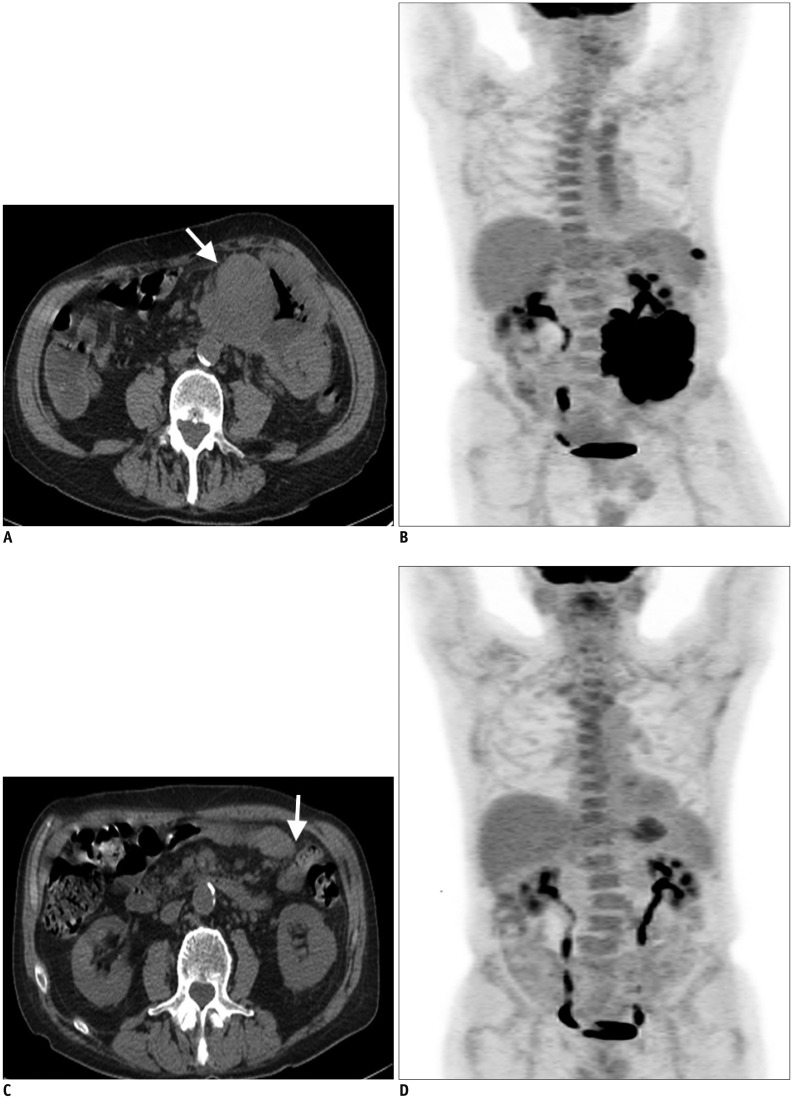
Diffuse large B cell lymphoma (DLBCL) is the most common histological subtype of Non-Hodgkin's lymphoma. As treatments continues to evolve, so do imaging strategies, and positron emission tomography (PET) has emerged as the most important imaging tool to guide oncologists in the diagnosis, staging, response assessment, relapse/recurrence detection,and therapeutic decision making of DLBCL. Other imaging modalities including magnetic resonance imaging (MRI), computed tomography (CT), ultrasound, and conventional radiography are also used in the evaluation of lymphoma. MRI is useful for nervous system and musculoskeletal system involvement and is emerging as a radiation free alternative to PET/CT. This article provides a comprehensive review of both the functional and morphological imaging modalities, available in the management of DLBCL.
Keywords: Diffuse large B cell lymphoma; FDG-positron emission tomography/CT; Lymphoma; MRI.
Figures


References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. - PubMed
-
- Møller MB, Pedersen NT, Christensen BE. Diffuse large B-cell lymphoma: clinical implications of extranodal versus nodal presentation--a population-based study of 1575 cases. Br J Haematol. 2004;124:151–159. - PubMed
-
- Shenoy PJ, Malik N, Nooka A, Sinha R, Ward KC, Brawley OW, et al. Racial differences in the presentation and outcomes of diffuse large B-cell lymphoma in the United States. Cancer. 2011;117:2530–2540. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
