

Review
doi: 10.3348/kjr.2017.18.1.71.
Epub 2017 Jan 5.
T-Cell Non-Hodgkin Lymphomas: Spectrum of Disease and the Role of Imaging in the Management of Common Subtypes
Affiliations
- PMID: 28096719
- PMCID: PMC5240486
- DOI: 10.3348/kjr.2017.18.1.71
Item in Clipboard
Review
T-Cell Non-Hodgkin Lymphomas: Spectrum of Disease and the Role of Imaging in the Management of Common Subtypes
Korean J Radiol.
2017 Jan-Feb.
Abstract
T-cell non-Hodgkin lymphomas (NHLs) are biologically diverse, uncommon malignancies characterized by a spectrum of imaging findings according to subtype. The purpose of this review is to describe the common subtypes of T-cell NHL, highlight important differences between cutaneous, various peripheral and precursor subtypes, and summarize imaging features and the role of imaging in the management of this diverse set of diseases.
Keywords: CT; MRI; Non-Hodgkin lymphoma; PET-CT; T-cell lymphoma.
Figures
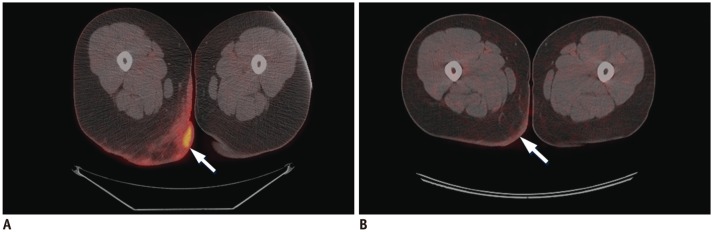
Baseline (A) and post treatment (B) axial fused PET-CT images demonstrate abnormal skin thickening in right posterior upper thigh/inferior buttock with associated intense 18FDG uptake (arrows), which resolved after treatment with radiation, photochemotherapy, and topical steroids. FDG = flourodeoxyglucose, PET = positron emission tomography

Axial contrast-enhanced CT image (A) demonstrates diffuse skin thickening in left groin (arrows), which resolved following treatment with radiation, phototherapy, and Targretin (not shown). Unfortunately, on subsequent restaging contrast-enhanced chest CT (B), patient developed bilateral pulmonary masses (arrows), which were biopsy proven cutaneous T-cell lymphoma. As seen on axial fused PET-CT image (C), pulmonary lesions increased in size and number despite treatment with cyclophosphamide, vincristine, doxorubicin, and prednisone (CHOP) regimen (arrow), pralatrexate, gemcitabine, Ontak, allogenic stem cell transplant, and palliative radiation and patient eventually expired from pulmonary complications. FDG = flourodeoxyglucose, PET = positron emission tomography
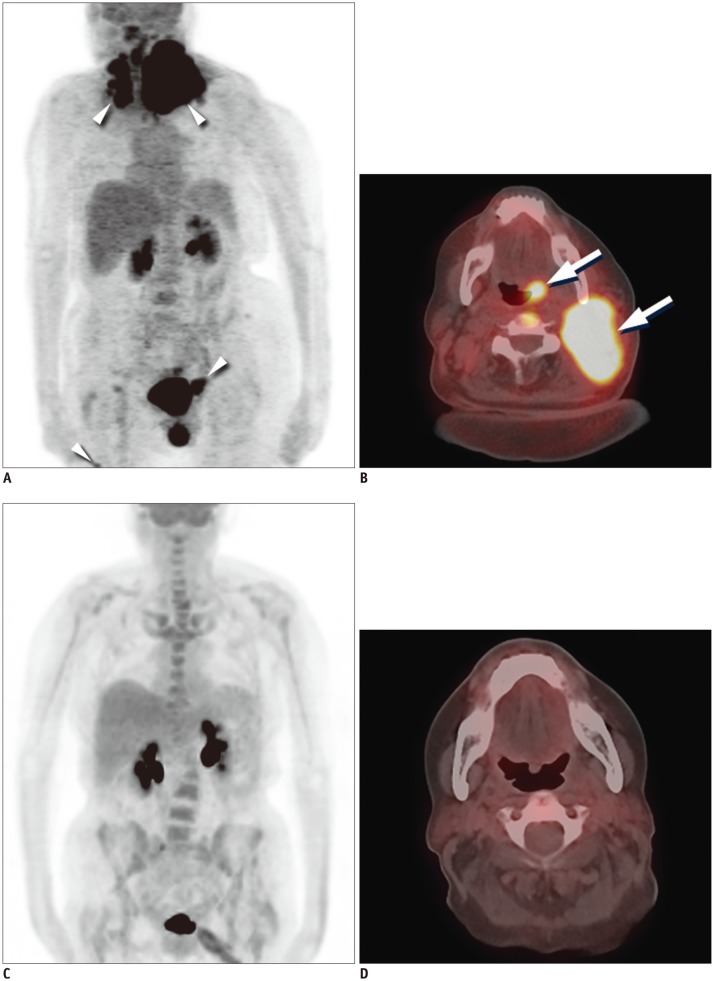
Baseline MIP (A) and axial fusion (B) PET-CT images demonstrate intense 18FDG uptake in left neck corresponding with large soft tissue mass and intense 18FDG uptake in left base of tongue (arrows). Additional sites of 18FDG uptake are seen in upper paratracheal region, inguinal stations, and right thigh (arrowheads). Post treatment MIP (C) and axial fusion (D) images following treatment with RCHOP and neck radiation demonstrate resolution of 18FDG uptake and soft tissue mass. FDG = flourodeoxyglucose, MIP = maximum intensity projection, PET = positron emission tomography
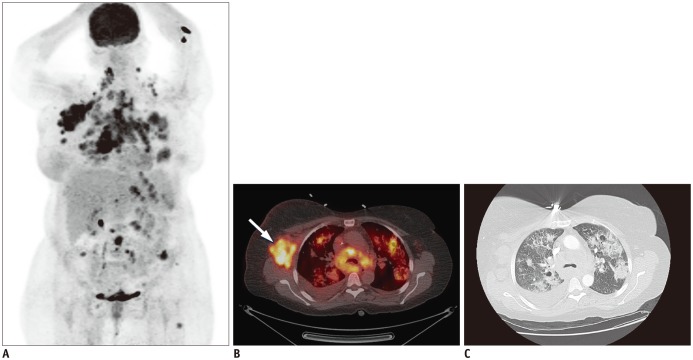
MIP image (A) demonstrates intense 18FDG uptake in cervical, thoracic, abdominal, and left inguinal lymph node stations, subcutaneous nodules, and bilateral pulmonary nodules, masses, and consolidations. Focal 18FDG uptakes in left arm are likely related to injection. Axial fused PET-CT image (B) demonstrates intense 18FDG uptake right axillary lymphadenopathy (arrow) and within bilateral pulmonary nodules and masses. Axial contrast-enhanced CT image on lung window (C) demonstrates pulmonary nodules and masses with surrounding groundglass opacities and mild intralobular septal thickening. One of lung masses was biopsied, and proven to be angioimmunoblastic lymphoma. Patient had complete response after treatment with CHOP and underwent autologous stem cell transplant but developed myelodysplastic syndrome and T-cell lymphoma recurrence and expired. FDG = flourodeoxyglucose, MIP = maximum intensity projection, PET = positron emission tomography
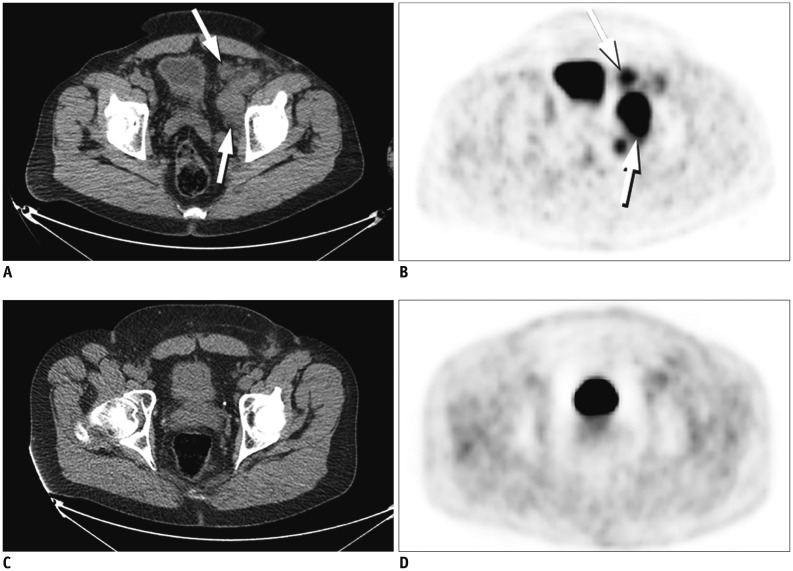
Baseline CT (A) and PET (B) images demonstrate intense 18FDG uptake within left external iliac and pelvic sidewall lymphadenopathy (arrows). Post treatment CT (C) and PET (D) images demonstrate complete resolution of lymphadenopathy and 18FDG uptake after treatment with CHOP. FDG = flourodeoxyglucose, PET = positron emission tomography
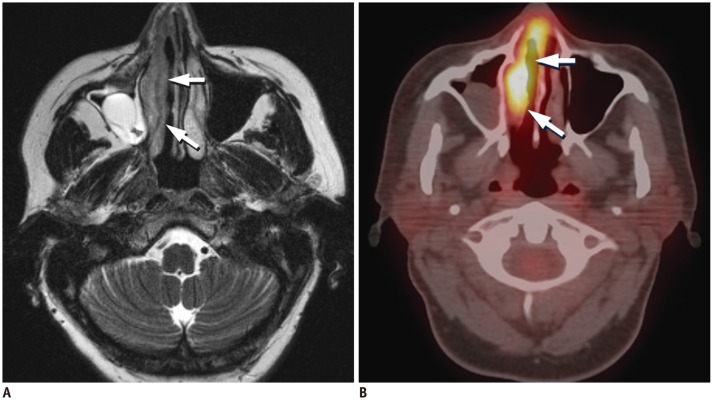
Axial T2-weighted MR image (A) shows diffuse thickening of right nasal mucosa with T2-hypointensity (arrows) compared to left side. Axial fused PET-CT image (B) demonstrates corresponding intense 18FDG uptake in right nasal cavity (arrows). FDG = flourodeoxyglucose, PET = positron emission tomography
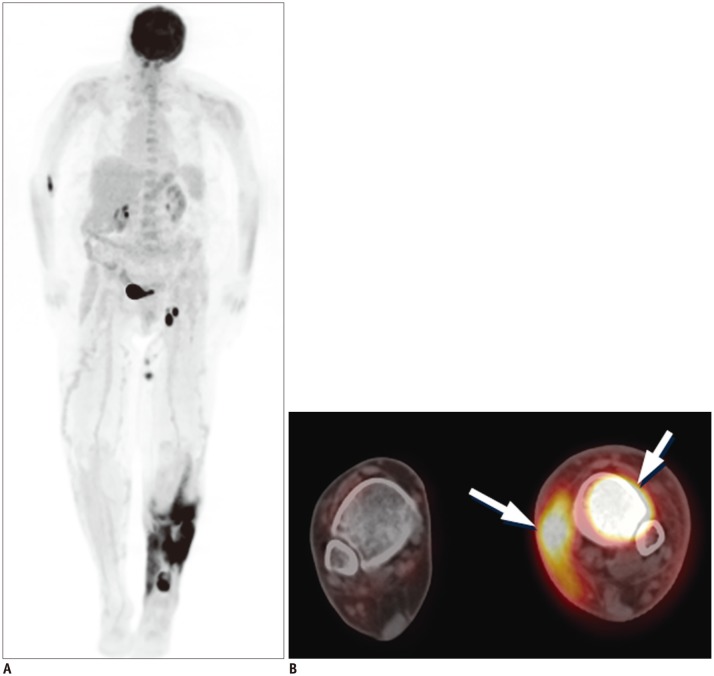
MIP (A) and axial fused PET-CT (B) images demonstrate intense 18FDG uptake in left lower extremity, involving marrow compartment of distal left tibia and surrounding subcutaneous soft tissue and overlying skin medially (arrows). FDG = flourodeoxyglucose, MIP = maximum intensity projection, PET = positron emission tomography
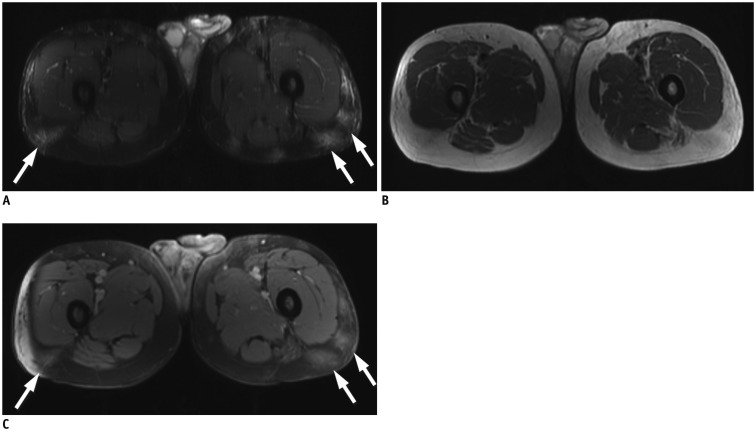
Axial T2 fat-sat (A) and T1-weighted (B) images demonstrate vague areas of increased T2 hyperintensity and T1 isointensity in subcutaneous tissues of posterior proximal thighs (arrows). Axial T1-weighted postcontrast (C) image demonstrates corresponding areas of enhancement (arrows).
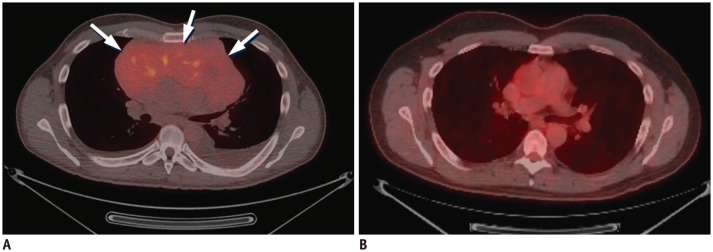
Baseline axial fused PET-CT image (A) demonstrates large hypo to isodense anterior mediastinal mass with mild to moderate 18FDG uptake (arrows). Post treatment axial fused PET-CT image (B) show resolution of anterior mediastinal mass and abnormal 18FDG uptake following treatment with Larson protocol intensification. FDG = flourodeoxyglucose, PET = positron emission tomography
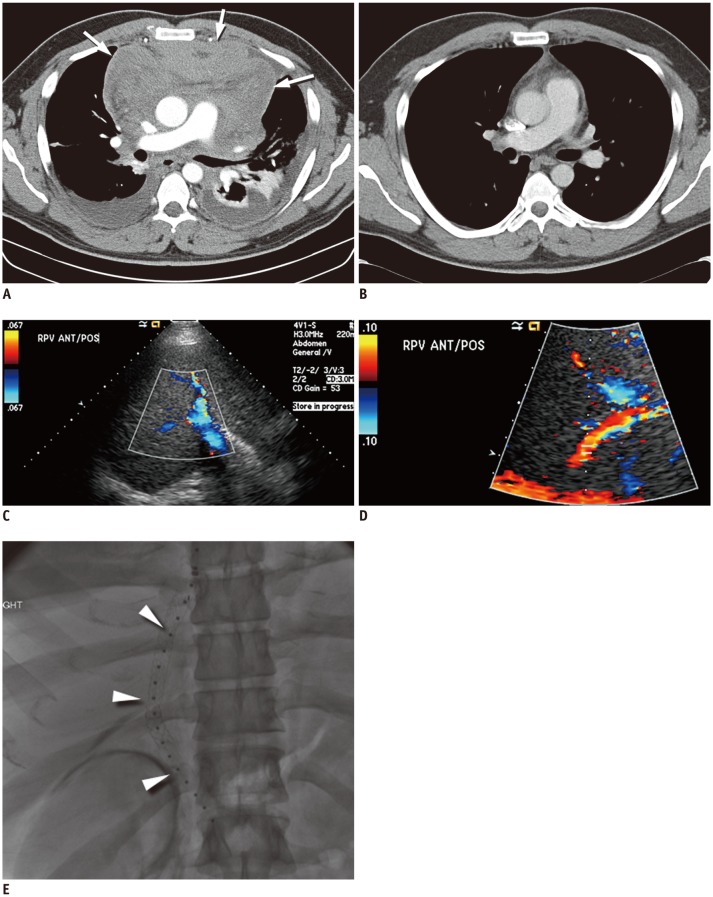
Baseline axial CT image (A) demonstrates large heterogeneously enhancing anterior mediastinal mass with associated pericardial effusion (arrows) and bilateral pleural effusions. Patient was taken for urgent pericardial window procedure, biopsy, which was initially thought to represent thymoma. Patient was treated with urgent radiation, chemotherapy with cytoxan, adriamycin, and cisplatin, and eventual surgical resection showing no residual disease in specimen, which was thought to be unusual for thymoma. Postsurgical axial CT image (B) demonstrates mild stranding in anterior mediastinum, consistent with postsurgical changes, without evidence for residual or recurrent lymphoma. Re-review of initial biopsy was felt to represent precursor T-cell lymphoma. Patient underwent induction chemotherapy per CALGB 9111 protocol and stem cell transplant. Following stem cell transplant, patient unfortunately developed veno-occlusive disease, as seen on ultrasound color Doppler images showing reversal of flow in right (C) and main (D) portal veins and expired despite transjugular intrahepatic portosystemic shunt procedure (arrowheads) (E).
References
-
- A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin's lymphoma. The Non-Hodgkin's Lymphoma Classification Project. Blood. 1997;89:3909–3918. - PubMed
-
- Vose J, Armitage J, Weisenburger D International T-Cell Lymphoma Project. International peripheral T-cell and natural killer/T-cell lymphoma study: pathology findings and clinical outcomes. J Clin Oncol. 2008;26:4124–4130. - PubMed
-
- Abouyabis AN, Shenoy PJ, Lechowicz MJ, Flowers CR. Incidence and outcomes of the peripheral T-cell lymphoma subtypes in the United States. Leuk Lymphoma. 2008;49:2099–2107. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
