

Diabetes Outpatient Care and Acute Complications Before and After High-Deductible Insurance Enrollment: A Natural Experiment for Translation in Diabetes (NEXT-D) Study
- PMID: 28097328
- PMCID: PMC5538022
- DOI: 10.1001/jamainternmed.2016.8411
Diabetes Outpatient Care and Acute Complications Before and After High-Deductible Insurance Enrollment: A Natural Experiment for Translation in Diabetes (NEXT-D) Study
Abstract
Importance: High-deductible health plans (HDHPs) have expanded under the Affordable Care Act and are expected to play a major role in the future of US health policy. The effects of modern HDHPs on chronically ill patients and adverse outcomes are unknown.
Objective: To determine the association of HDHP with high-priority diabetes outpatient care and preventable acute complications.
Design, setting, and participants: Controlled interrupted-time-series study using a large national health insurer database from January 1, 2003, to December 31, 2012. A total of 12 084 HDHP members with diabetes, aged 12 to 64 years, who were enrolled for 1 year in a low-deductible (≤$500) plan followed by 2 years in an HDHP (≥$1000) after an employer-mandated switch were included. Patients transitioning to HDHPs were propensity-score matched with contemporaneous patients whose employers offered only low-deductible coverage. Low-income (n = 4121) and health savings account (HSA)-eligible (n = 1899) patients with diabetes were subgroups of interest. Data analysis was performed from February 23, 2015, to September 11, 2016.
Exposures: Employer-mandated HDHP transition.
Main outcomes and measures: High-priority outpatient visits, disease monitoring tests, and outpatient and emergency department visits for preventable acute diabetes complications.
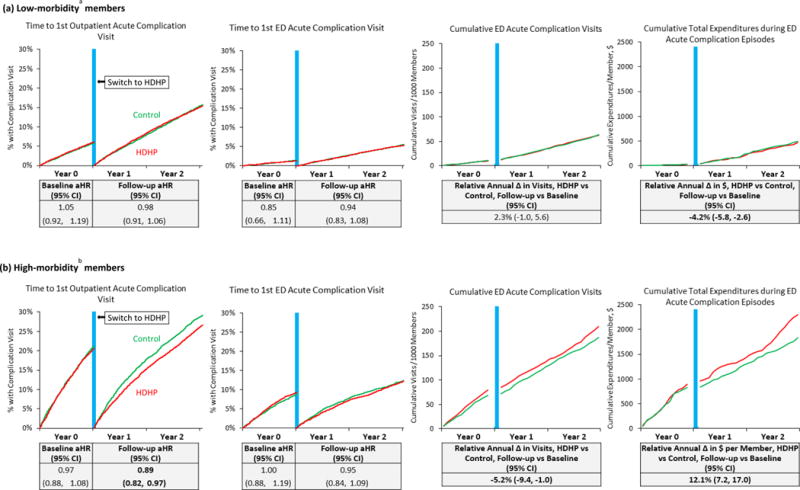
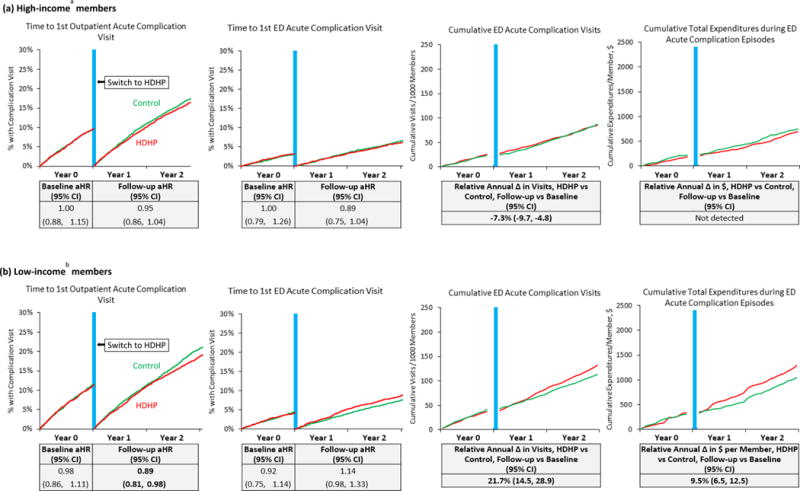
Results: In the 12 084 HDHP members included after the propensity score match, the mean (SD) age was 50.4 (10.0) years; 5410 of the group (44.8%) were women. The overall, low-income, and HSA-eligible diabetes HDHP groups experienced increases in out-of-pocket medical expenditures of 49.4% (95% CI, 40.3% to 58.4%), 51.7% (95% CI, 38.6% to 64.7%), and 67.8% (95% CI, 47.9% to 87.8%), respectively, compared with controls in the year after transitioning to HDHPs. High-priority primary care visits and disease monitoring tests did not change significantly in the overall HDHP cohort; however, high-priority specialist visits declined by 5.5% (95% CI, -9.6% to -1.5%) in follow-up year 1 and 7.1% (95% CI, -11.5% to -2.7%) in follow-up year 2 vs baseline. Outpatient acute diabetes complication visits were delayed in the overall and low-income HDHP cohorts at follow-up (adjusted hazard ratios, 0.94 [95% CI, 0.88 to 0.99] for the overall cohort and 0.89 [95% CI, 0.81 to 0.98] for the low-income cohort). Annual emergency department acute complication visits among HDHP members increased by 8.0% (95% CI, 4.6% to 11.4%) in the overall group, 21.7% (95% CI, 14.5% to 28.9%) in the low-income group, and 15.5% (95% CI, 10.5% to 20.6%) in the HSA-eligible group.
Conclusions and relevance: Patients with diabetes experienced minimal changes in outpatient visits and disease monitoring after an HDHP switch, but low-income and HSA-eligible HDHP members experienced major increases in emergency department visits for preventable acute diabetes complications.
Conflict of interest statement
CONFLICTS OF INTEREST/FINANCIAL DISCLOSURES:
The authors have no conflicts of interest or financial disclosures to report.
Figures
Comment in
-
Precision Benefit Design-Using "Smarter" Deductibles to Better Engage Consumers and Mitigate Cost-Related Nonadherence.JAMA Intern Med. 2017 Mar 1;177(3):368-370. doi: 10.1001/jamainternmed.2016.8747. JAMA Intern Med. 2017. PMID: 28097300 No abstract available.
References
-
- The Kaiser Family Foundation and Health Research & Educational Trust 2015 Annual Survey Employer Health Benefits. 2015 http://files.kff.org/attachment/summary-of-findings-2015-employer-health.... Accessed 24 September, 2015.
-
- Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics–2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119(3):480–486. - PubMed
-
- Hu FB, Stampfer MJ, Solomon CG, et al. The impact of diabetes mellitus on mortality from all causes and coronary heart disease in women: 20 years of follow-up. Arch Intern Med. 2001;161(14):1717–1723. - PubMed
-
- Schreyogg J, Stargardt T, Tiemann O. Costs and quality of hospitals in different health care systems: a multi-level approach with propensity score matching. Health Econ. 2011;20(1):85–100. - PubMed
-
- Cook EF, Goldman L. Performance of tests of significance based on stratification by a multivariate confounder score or by a propensity score. Journal of clinical epidemiology. 1989;42(4):317–324. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
