

Effect of Incentive Spirometry on Postoperative Hypoxemia and Pulmonary Complications After Bariatric Surgery: A Randomized Clinical Trial
- PMID: 28097332
- PMCID: PMC5831447
- DOI: 10.1001/jamasurg.2016.4981
Effect of Incentive Spirometry on Postoperative Hypoxemia and Pulmonary Complications After Bariatric Surgery: A Randomized Clinical Trial
Abstract
Importance: The combination of obesity and foregut surgery puts patients undergoing bariatric surgery at high risk for postoperative pulmonary complications. Postoperative incentive spirometry (IS) is a ubiquitous practice; however, little evidence exists on its effectiveness.
Objective: To determine the effect of postoperative IS on hypoxemia, arterial oxygen saturation (Sao2) level, and pulmonary complications after bariatric surgery.
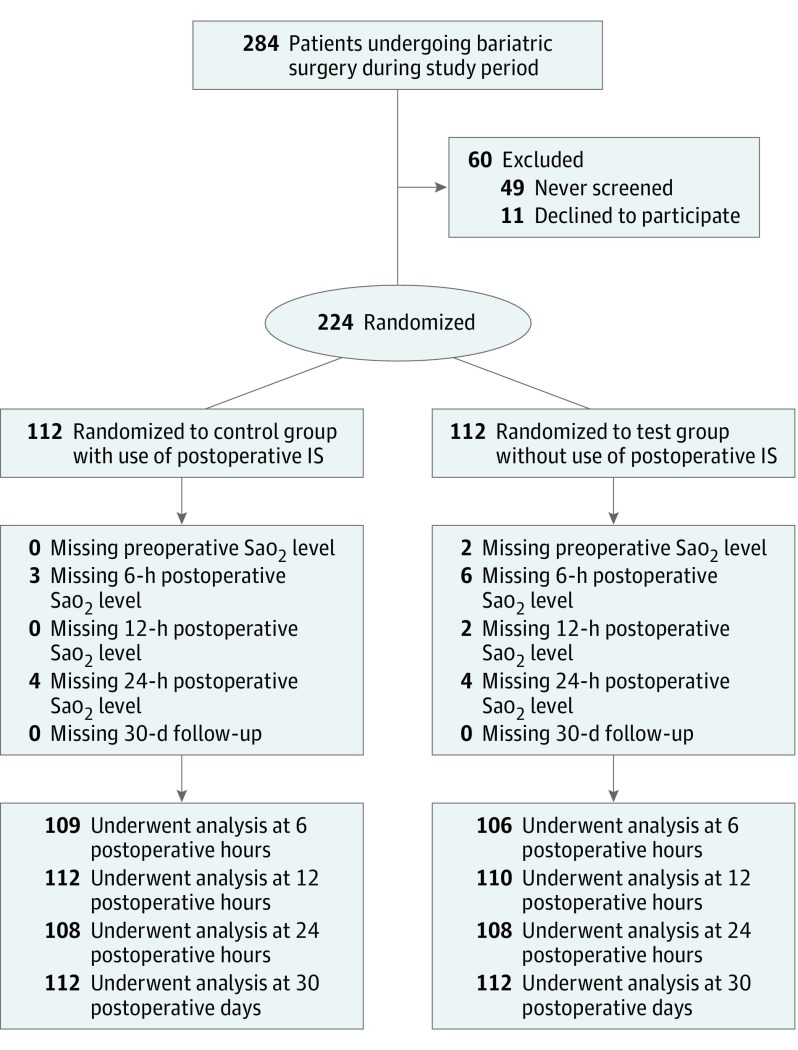
Design, setting, and participants: A randomized noninferiority clinical trial enrolled patients undergoing bariatric surgery from May 1, 2015, to June 30, 2016. Patients were randomized to postoperative IS (control group) or clinical observation (test group) at a single-center tertiary referral teaching hospital. Analysis was based on the evaluable population.
Interventions: The controls received the standard of care with IS use 10 times every hour while awake. The test group did not receive an IS device or these orders.
Main outcomes and measures: The primary outcome was frequency of hypoxemia, defined as an Sao2 level of less than 92% without supplementation at 6, 12, and 24 postoperative hours. Secondary outcomes were Sao2 levels at these times and the rate of 30-day postoperative pulmonary complications.
Results: A total of 224 patients (50 men [22.3%] and 174 women [77.7%]; mean [SD] age, 45.6 [11.8] years) were enrolled, and 112 were randomized for each group. Baseline characteristics of the groups were similar. No significant differences in frequency of postoperative hypoxemia between the control and test groups were found at 6 (11.9% vs 10.4%; P = .72), 12 (5.4% vs 8.2%; P = .40), or 24 (3.7% vs 4.6%; P = .73) postoperative hours. No significant differences were observed in mean (SD) Sao2 level between the control and test groups at 6 (94.9% [3.2%] vs 94.9% [2.9%]; P = .99), 12 (95.4% [2.2%] vs 95.1% [2.5%]; P = .40), or 24 (95.7% [2.4%] vs 95.6% [2.4%]; P = .69) postoperative hours. Rates of 30-day postoperative pulmonary complications did not differ between groups (8 patients [7.1%] in the control group vs 4 [3.6%] in the test group; P = .24).
Conclusions and relevance: Postoperative IS did not demonstrate any effect on postoperative hypoxemia, Sao2 level, or postoperative pulmonary complications. Based on these findings, the routine use of IS is not recommended after bariatric surgery in its current implementation.
Trial registration: clinicaltrials.gov Identifier: NCT02431455.
Conflict of interest statement
Figures
Comment in
-
Incentive Spirometry After Bariatric Surgery: Yes or No?JAMA Surg. 2017 May 1;152(5):428. doi: 10.1001/jamasurg.2016.4999. JAMA Surg. 2017. PMID: 28097336 No abstract available.
-
Incentive Spirometry After Bariatric Surgery-Reply.JAMA Surg. 2017 Oct 1;152(10):985-986. doi: 10.1001/jamasurg.2017.1678. JAMA Surg. 2017. PMID: 28636696 No abstract available.
-
Incentive Spirometry After Bariatric Surgery: The Importance of Patient Compliance.JAMA Surg. 2017 Oct 1;152(10):984-985. doi: 10.1001/jamasurg.2017.1698. JAMA Surg. 2017. PMID: 28636722 Free PMC article. No abstract available.
References
-
- World Health Organization. Obesity and overweight. http://www.who.int/mediacentre/factsheets/fs311/en/. Udpated June 2016. Accessed December 8, 2016.
-
- Angrisani L, Santonicola A, Iovino P, Formisano G, Buchwald H, Scopinaro N. Bariatric surgery worldwide 2013. Obes Surg. 2015;25(10):1822-1832. - PubMed
-
- Pasulka PS, Bistrian BR, Benotti PN, Blackburn GL. The risks of surgery in obese patients. Ann Intern Med. 1986;104(4):540-546. - PubMed
-
- Rothen HU, Sporre B, Engberg G, Wegenius G, Hedenstierna G. Airway closure, atelectasis and gas exchange during general anaesthesia. Br J Anaesth. 1998;81(5):681-686. - PubMed
-
- Overend TJ, Anderson CM, Lucy SD, Bhatia C, Jonsson BI, Timmermans C. The effect of incentive spirometry on postoperative pulmonary complications: a systematic review. Chest. 2001;120(3):971-978. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
