

Deletion of Nlrp3 protects from inflammation-induced skeletal muscle atrophy
- PMID: 28097512
- PMCID: PMC5241267
- DOI: 10.1186/s40635-016-0115-0
Deletion of Nlrp3 protects from inflammation-induced skeletal muscle atrophy
Abstract
Background: Critically ill patients develop atrophic muscle failure, which increases morbidity and mortality. Interleukin-1β (IL-1β) is activated early in sepsis. Whether IL-1β acts directly on muscle cells and whether its inhibition prevents atrophy is unknown. We aimed to investigate if IL-1β activation via the Nlrp3 inflammasome is involved in inflammation-induced atrophy.
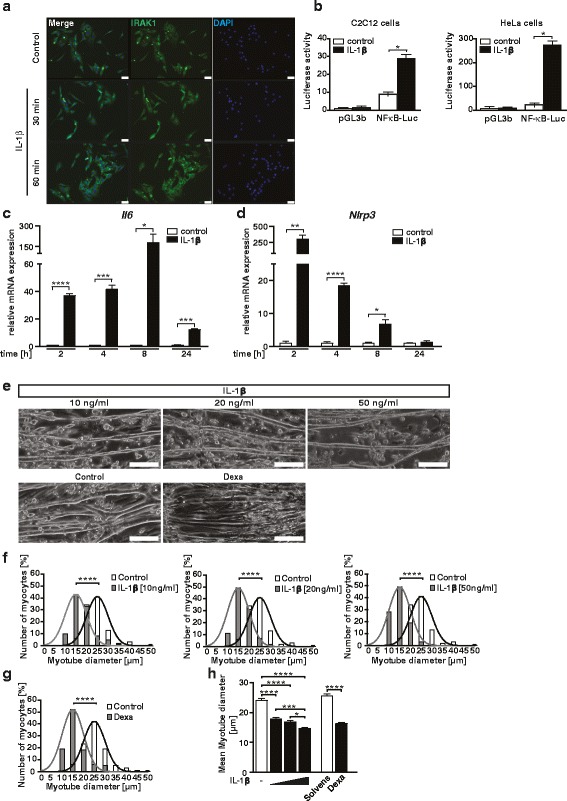
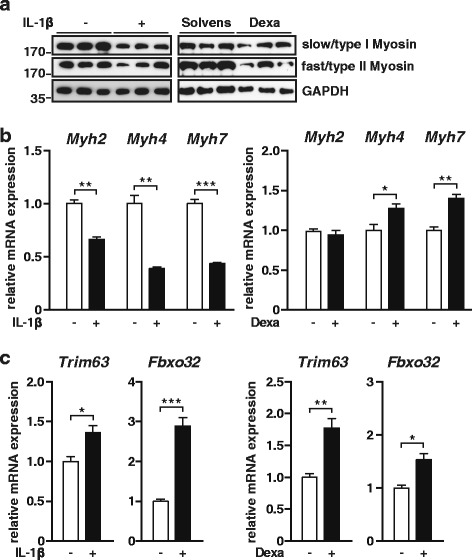
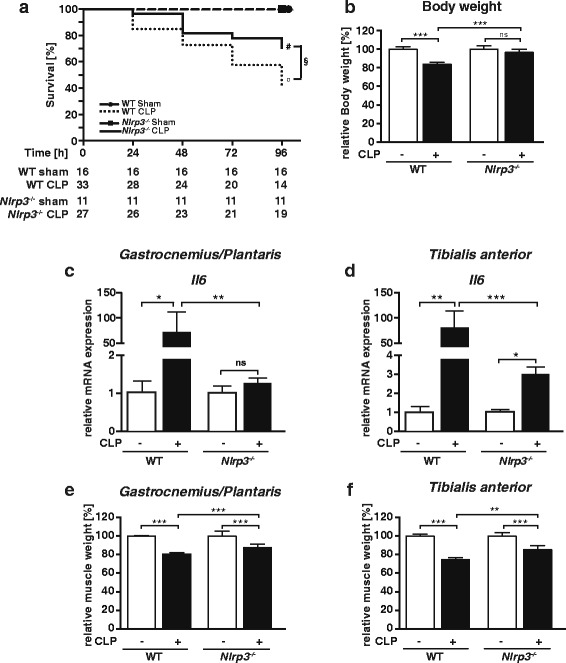
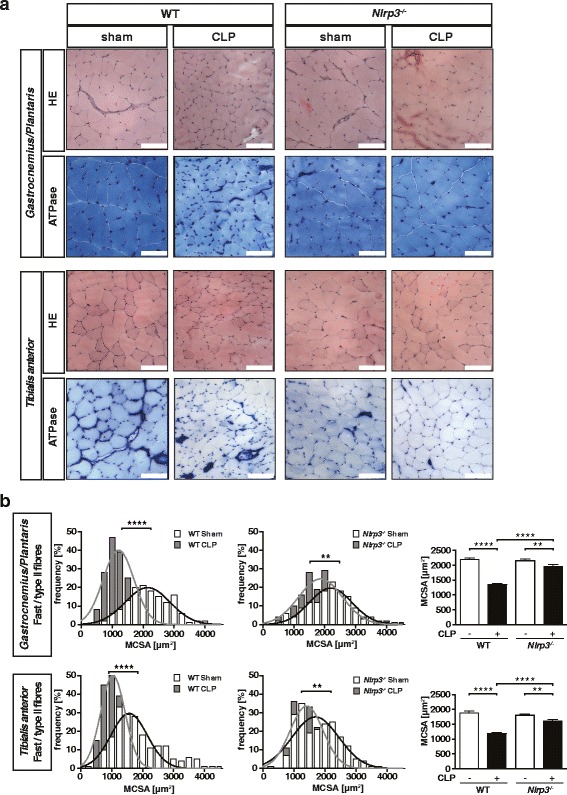
Methods: We performed an experimental study and prospective animal trial. The effect of IL-1β on differentiated C2C12 muscle cells was investigated by analyzing gene-and-protein expression, and atrophy response. Polymicrobial sepsis was induced by cecum ligation and puncture surgery in Nlrp3 knockout and wild type mice. Skeletal muscle morphology, gene and protein expression, and atrophy markers were used to analyze the atrophy response. Immunostaining and reporter-gene assays showed that IL-1β signaling is contained and active in myocytes.
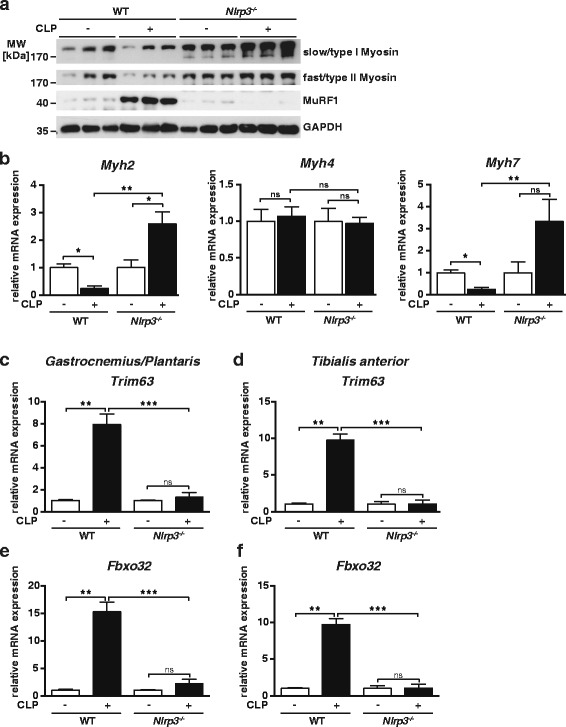
Results: Immunostaining and reporter gene assays showed that IL-1β signaling is contained and active in myocytes. IL-1β increased Il6 and atrogene gene expression resulting in myocyte atrophy. Nlrp3 knockout mice showed reduced IL-1β serum levels in sepsis. As determined by muscle morphology, organ weights, gene expression, and protein content, muscle atrophy was attenuated in septic Nlrp3 knockout mice, compared to septic wild-type mice 96 h after surgery.
Conclusions: IL-1β directly acts on myocytes to cause atrophy in sepsis. Inhibition of IL-1β activation by targeting Nlrp3 could be useful to prevent inflammation-induced muscle failure in critically ill patients.
Keywords: ICUAW; IL-1β; Muscle weakness; Sepsis.
Figures
References
-
- Bierbrauer J, Koch S, Olbricht C, Hamati J, Lodka D, Schneider J, Luther-Schröder A, Kleber C, Faust K, Wiesener S, Spies CD, Spranger J, Spuler S, Fielitz J, Weber-Carstens S. Early type II fiber atrophy in intensive care unit patients with nonexcitable muscle membrane. Crit Care Med. 2012;40:647–650. doi: 10.1097/CCM.0b013e31823295e6. - DOI - PubMed
-
- Puthucheary ZA, Rawal J, McPhail M, Connolly B, Ratnayake G, Chan P, Hopkinson NS, Phadke R, Padhke R, Dew T, Sidhu PS, Velloso C, Seymour J, Agley CC, Selby A, Limb M, Edwards LM, Smith K, Rowlerson A, Rennie MJ, Moxham J, Harridge SDR, Hart N, Montgomery HE. Acute skeletal muscle wasting in critical illness. JAMA. 2013;310:1591–1600. doi: 10.1001/jama.2013.278481. - DOI - PubMed
-
- De Jonghe B, Sharshar T, Lefaucheur J-P, Authier F-J, Durand-Zaleski I, Boussarsar M, Cerf C, Renaud E, Mesrati F, Carlet J, Raphaël J-C, Outin H, Bastuji-Garin S, Groupe de Réflexion et d’Etude des Neuromyopathies en R Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA. 2002;288:2859–2867. doi: 10.1001/jama.288.22.2859. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
