

Regional Differences in the Prescription of Biologics for Psoriasis in Sweden: A Register-Based Study of 4168 Patients
- PMID: 28097638
- PMCID: PMC5258782
- DOI: 10.1007/s40259-016-0209-y
Regional Differences in the Prescription of Biologics for Psoriasis in Sweden: A Register-Based Study of 4168 Patients
Abstract
Background: Observational studies suggest an inequitable prescription of biologics in psoriasis care, which may be attributed to geographical differences in treatment access. Sweden regularly ranks high in international comparisons of equitable healthcare, and is, in connection with established national registries, an ideal country to investigate potential inequitable access.
Objective: The aim was to determine whether the opportunity for patients to receive biologics depends on where they receive care.
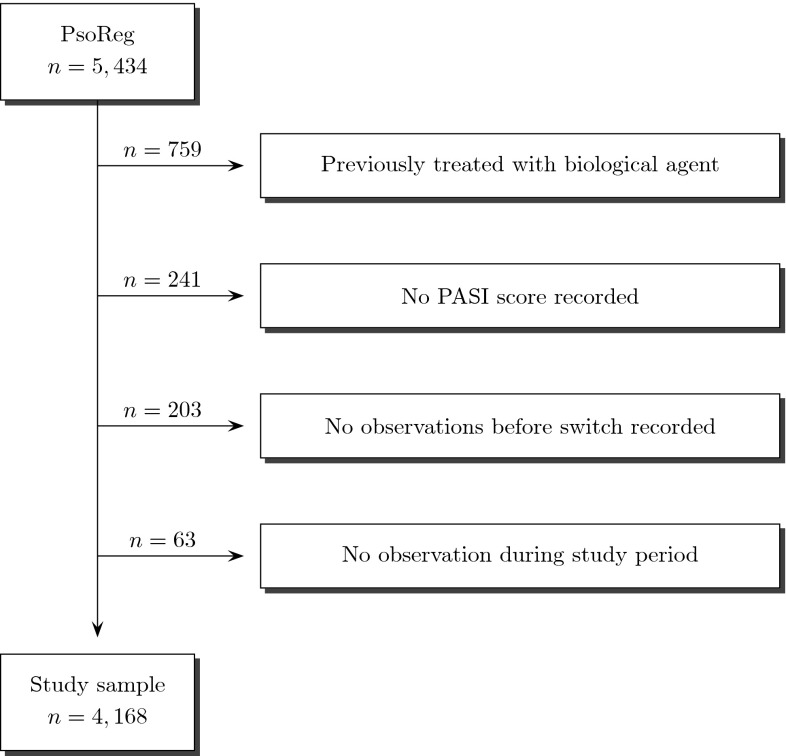
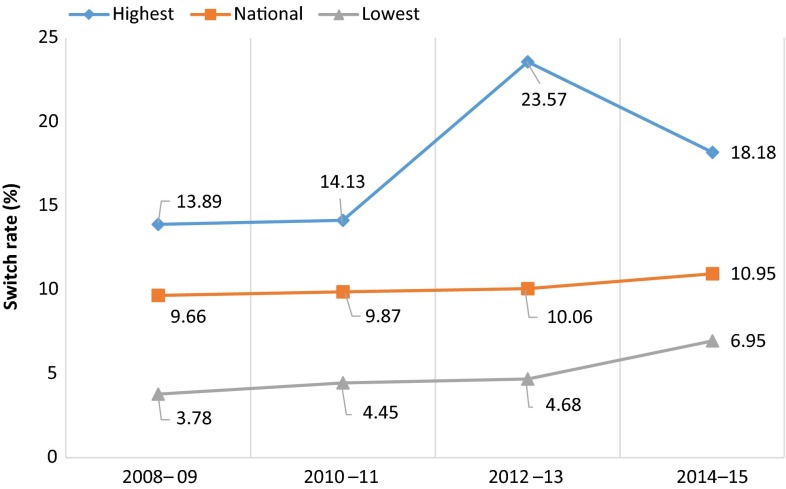
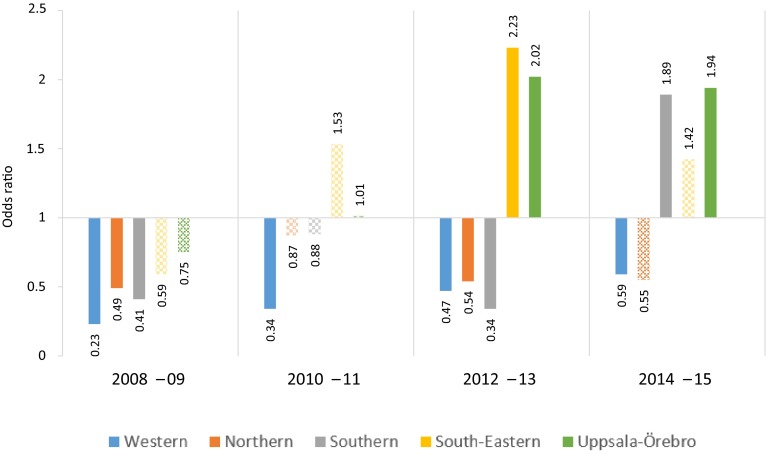
Methods: Biologic-naïve patients enrolled in the Swedish National Register for Systemic Treatment of Psoriasis (PsoReg) from 2008 to 2015 (n = 4168) were included. The association between the likelihood of initiating a biologic and the region where patients received care was analyzed. The strength of the association was adjusted for patient and clinical characteristics, as well as disease severity using logistic regression analysis. The proportion of patients that switched to a biologic (switch rate) and the probability of switch to a biologic was calculated in 2-year periods.
Results: The national switch rate increased marginally over time from 9.7 to 11.0%, though the uptake varied across regions. Adjusted odds ratios for at least one region were significantly different from the reference region in every 2-year period. During the latest period (2014-2015), the average patient in the lowest prescribing region was nearly 2.5 times less likely to switch as a similar patient in the highest prescribing region.
Conclusions: Geographical differences in biologics prescription persist after adjusting for patient characteristics and disease severity. The Swedish example calls for further improvements in delivering equitable psoriasis care.
Conflict of interest statement
Compliance with ethical standardsEthical approvalsResearch was done in adherence with the Declaration of Helsinki, and the study was approved by the Umeå Ethical Review Board. Patients were recruited after informed consent was obtained. Both data and consent were collected electronically to ensure an effective logistic in this nationwide project.FundingPsoReg receives financial support from the Swedish Board of Health and Welfare, Swedish Association of Local Authorities and Regions, and Västerbotten County Council. The research has received financial support from Abbvie, Janssen Cilag, Leo Pharma, Novartis, and Pfizer. Sponsors had no access to data. The authors had full independence regarding data collection, manuscript preparation, decision to publish, study design, interpretation, and analysis.Conflict of interestM. Schmitt-Egenolf is the manager of PsoReg and responsible for dermatology in the project management for the national guidelines for psoriasis at the Swedish Board of Health and Welfare. P. S. Calara, R. Althin, K. Steen Carlsson have no further conflicts of interest to declare.
Figures
References
-
- Lofvendahl S, Theander E, Svensson A, Carlsson KS, Englund M, Petersson IF. Validity of diagnostic codes and prevalence of physician-diagnosed psoriasis and psoriatic arthritis in southern Sweden—a population-based register study. PLoS One. 2014;9(5):e98024. doi: 10.1371/journal.pone.0098024. - DOI - PMC - PubMed
-
- Parisi R, Symmons DP, Griffiths CE, Ashcroft DM, Identification and Management of Psoriasis and Associated ComorbidiTy (IMPACT) Project Team et al. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133(2):377–385. doi: 10.1038/jid.2012.339. - DOI - PubMed
-
- Brandrup F, Green A. The prevalence of psoriasis in Denmark. Acta Derm Venereol. 1981;61(4):344–346. - PubMed
-
- Hägg D. Psoriasis in Sweden: observational studies from an epidemiological perspective. Umeå: Umeå University; 2016.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
