

Changing Epidemiology of Human Brucellosis, China, 1955-2014
- PMID: 28098531
- PMCID: PMC5324817
- DOI: 10.3201/eid2302.151710
Changing Epidemiology of Human Brucellosis, China, 1955-2014
Abstract
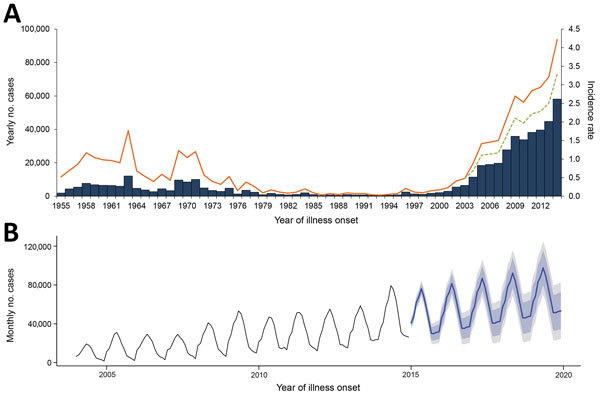
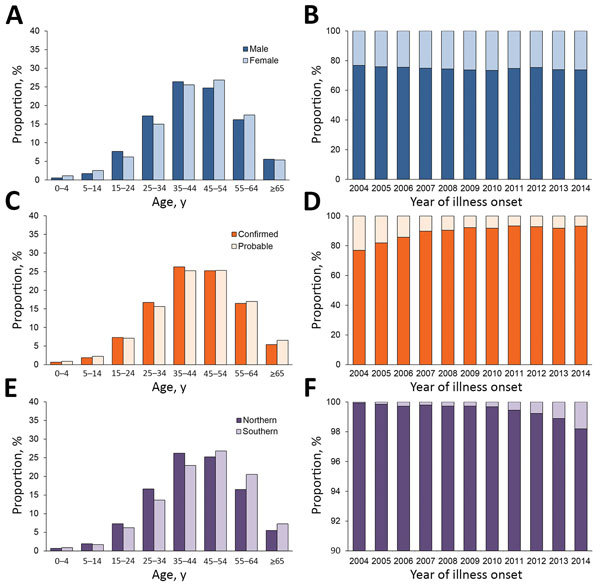
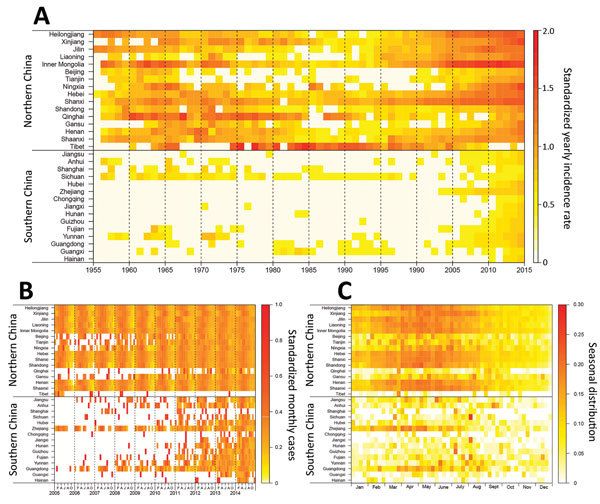
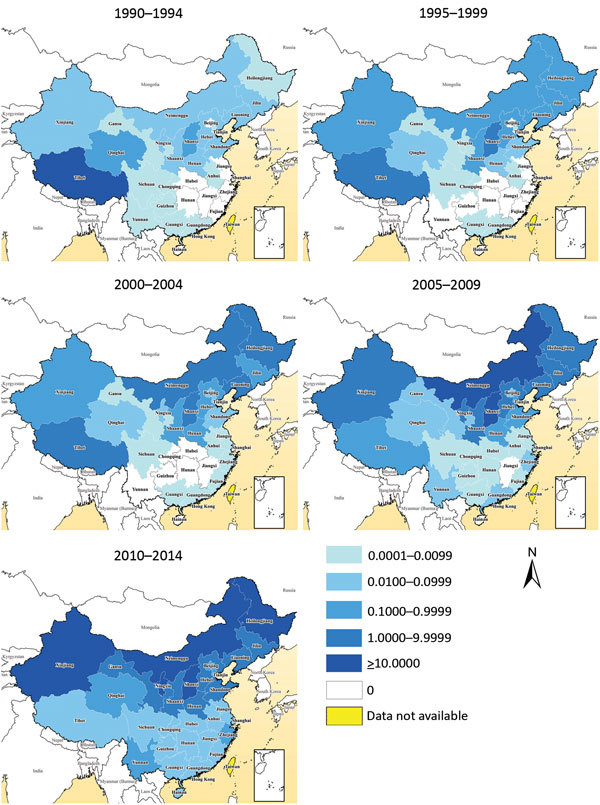
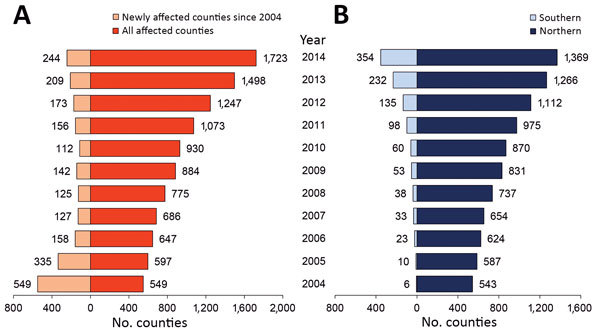
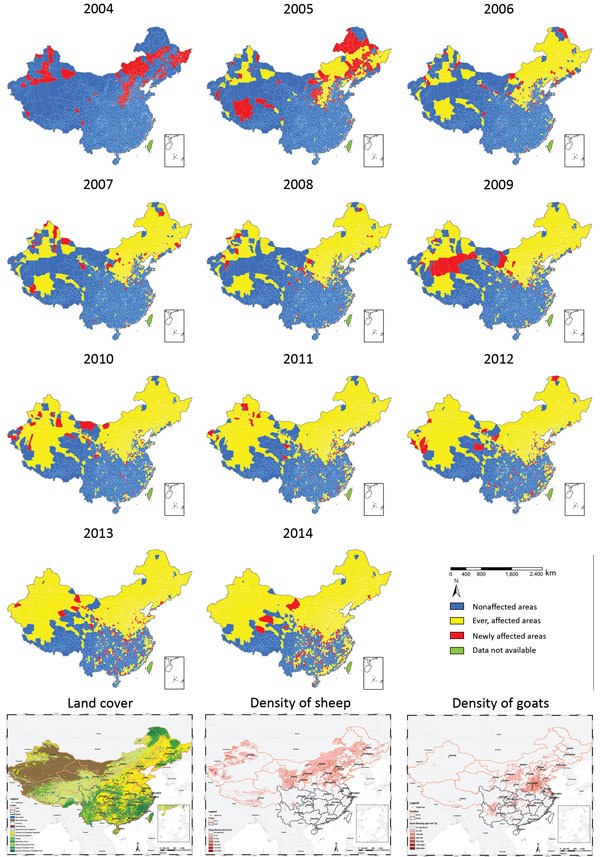
Brucellosis, a zoonotic disease, was made statutorily notifiable in China in 1955. We analyzed the incidence and spatial-temporal distribution of human brucellosis during 1955-2014 in China using notifiable surveillance data: aggregated data for 1955-2003 and individual case data for 2004-2014. A total of 513,034 brucellosis cases were recorded, of which 99.3% were reported in northern China during 1955-2014, and 69.1% (258, 462/374, 141) occurred during February-July in 1990-2014. Incidence remained high during 1955-1978 (interquartile range 0.42-1.0 cases/100,000 residents), then decreased dramatically in 1979-1994. However, brucellosis has reemerged since 1995 (interquartile range 0.11-0.23 in 1995-2003 and 1.48-2.89 in 2004-2014); the historical high occurred in 2014, and the affected area expanded from northern pastureland provinces to the adjacent grassland and agricultural areas, then to southern coastal and southwestern areas. Control strategies in China should be adjusted to account for these changes by adopting a One Health approach.
Keywords: Brucella; Brucellosis; China; bacteria; epidemiology; humans; zoonoses.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
