

Building personalized treatment plans for early-stage colorectal cancer patients
- PMID: 28099153
- PMCID: PMC5355140
- DOI: 10.18632/oncotarget.14638
Building personalized treatment plans for early-stage colorectal cancer patients
Abstract
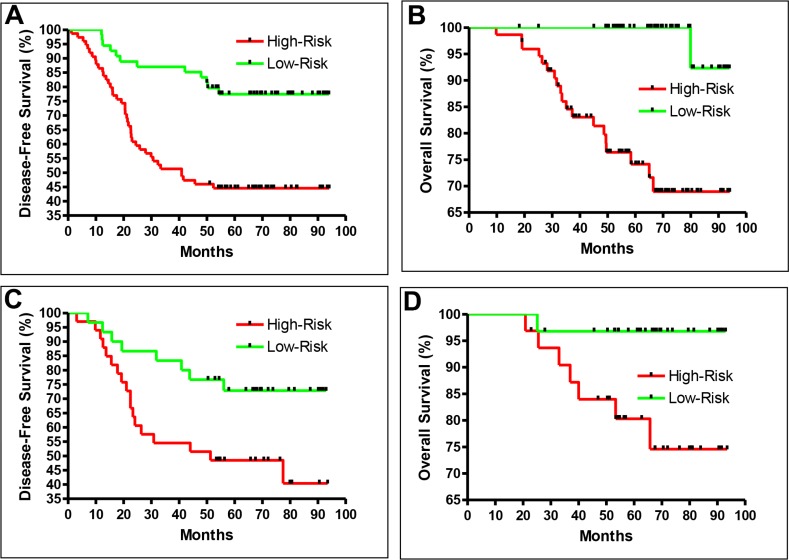
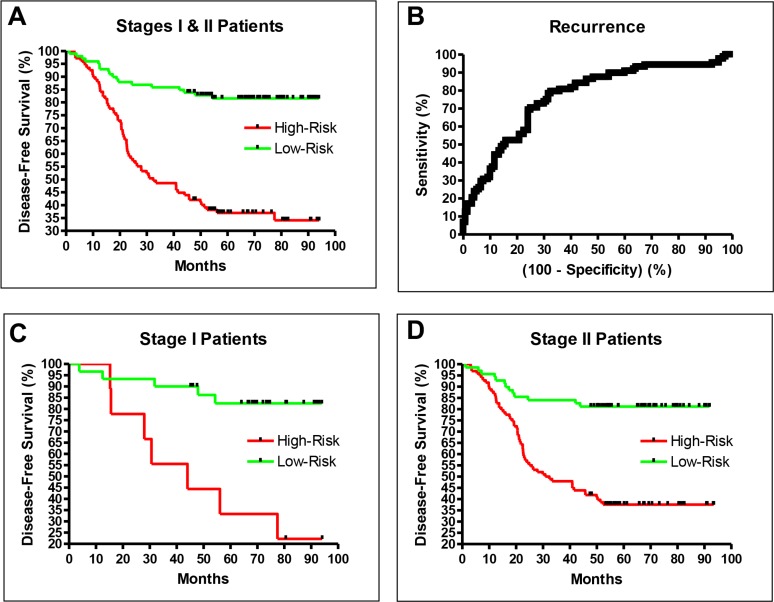
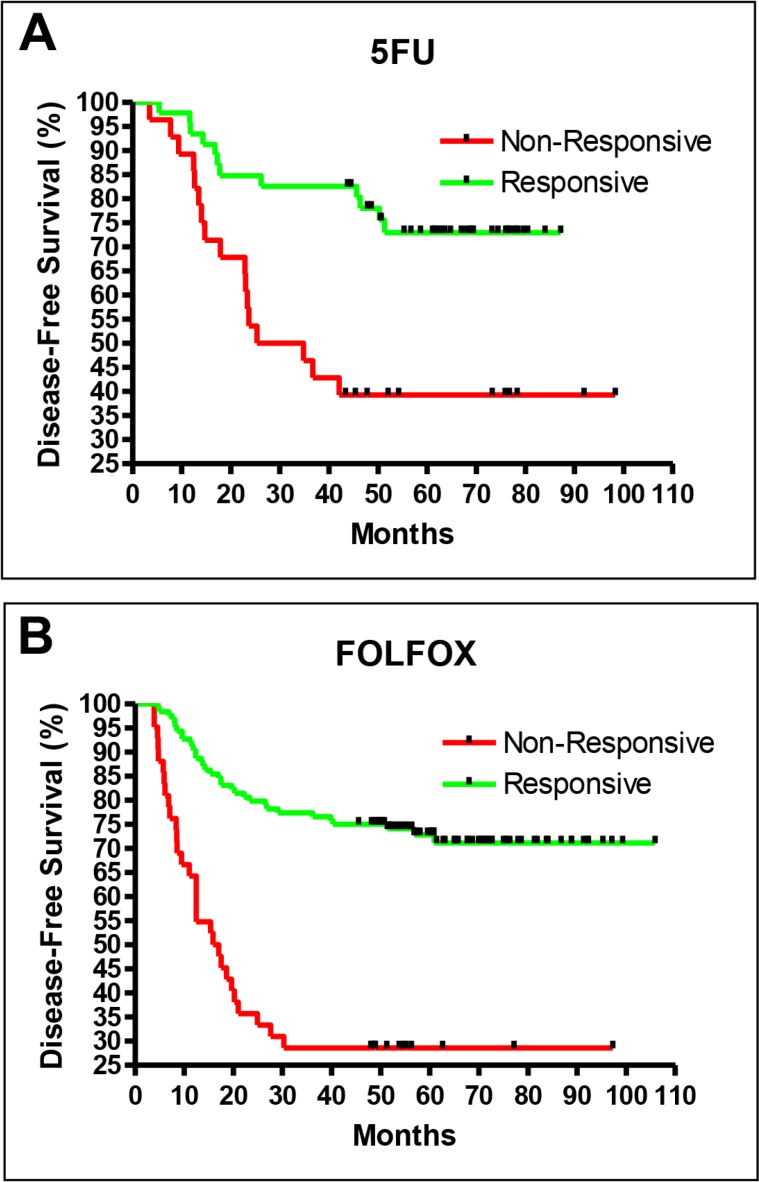
We developed a series of models to predict the likelihood of recurrence and the response to chemotherapy for the personalized treatment of stage I and II colorectal cancer patients. A recurrence prediction model was developed from 235 stage I/II patients. The model successfully distinguished between high-risk and low-risk groups, with a hazard ratio of recurrence of 4.66 (p < 0.0001). More importantly, the model was accurate for both stage I (hazard ratio = 5.87, p = 0.0006) and stage II (hazard ratio = 4.30, p < 0.0001) disease. This model performed much better than the Oncotype and ColoPrint commercial services in identifying patients at high risk for stage II recurrence. And unlike the commercial services, the robust model included recurrence prediction for stage I patients. As stage I/II CRC patients usually do not receive chemotherapy, we generated chemotherapy efficacy prediction models with data from 358 stage III patients. The predictions were highly accurate: the hazard ratio of recurrence for responders vs. non-responders was 4.13 for those treated with FOLFOX (p < 0.0001), and 3.16 (p = 0.0012) for those treated with fluorouracil. We have thus created a prognostic model that accurately identifies patients at high risk for recurrence, and the first accurate chemotherapy efficacy prediction model for individual patients. In the future, complete personalized treatment plans for stage I/II patients may be developed if the drug prediction models generated from stage III patients are verified to be effective for stage I and II patients in prospective studies.
Keywords: colorectal cancer; drug efficacy; microarray; personalized treatment; recurrence.
Conflict of interest statement
N Wei owns company stocks. No potential conflicts of interest were disclosed by the other authors.
Figures
References
-
- Wilkinson NW, Yothers G, Lopa S, Costantino JP, Petrelli NJ, Wolmark N. Long-Term Survival Results of Surgery Alone Versus Surgery Plus 5-Fluorouracil and Leucovorin for Stage II and Stage III Colon Cancer: Pooled Analysis of NSABP C-01 Through C-05. A Baseline from Which to Compare Modern Adjuvant Trials. Ann Surg Oncol. 2010;17:959–66. - PMC - PubMed
-
- Sargent DJ, Patiyil S, Yothers G, Haller DG, Gray R, Benedetti J, Buyse M, Labianca R, Seitz JF, O'Callaghan CJ, Francini G, Grothey A, O'Connell M, et al. End points for colon cancer adjuvant trials: Observations and recommendations based on individual patient data from 20,898 patients enrolled onto 18 randomized trials from the ACCENT group. J Clin Oncol. 2007;25:4569–74. - PubMed
-
- Manfredi S, Bouvier AM, Lepage C, Hatem C, Dancourt V, Faivre J. Incidence and patterns of recurrence after resection for cure of colonic cancer in a well defined population. Br J Surg. 2006;93:1115–22. - PubMed
-
- Howlader N, Noone A, Krapcho M, Garshell J, Miller D, Altekruse S, Kosary C, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis D, Chen H, et al. SEER Cancer Statistics Review, 1975–2012, National Cancer Institute. Bethesda, MD.: 2015.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
