

Dysfunctional tear syndrome: dry eye disease and associated tear film disorders - new strategies for diagnosis and treatment
- PMID: 28099212
- PMCID: PMC5345890
- DOI: 10.1097/01.icu.0000512373.81749.b7
Dysfunctional tear syndrome: dry eye disease and associated tear film disorders - new strategies for diagnosis and treatment
Abstract
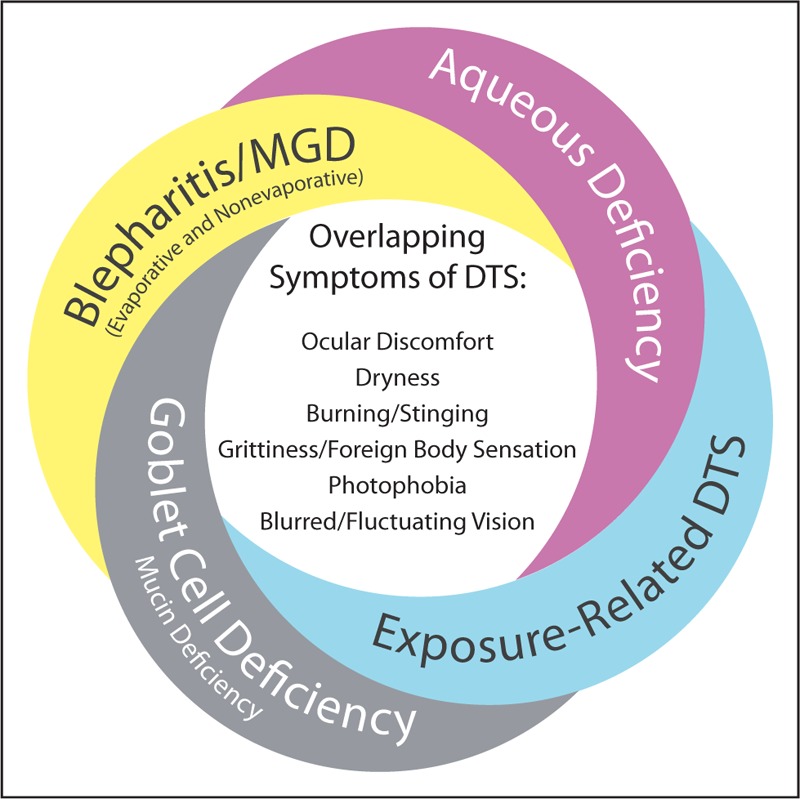
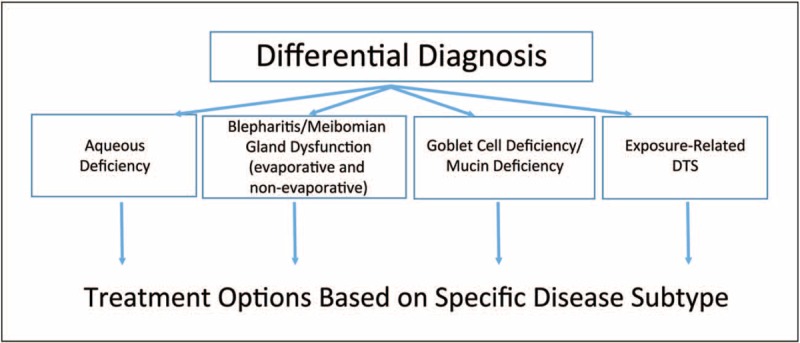
Dysfunctional tear syndrome (DTS) is a common and complex condition affecting the ocular surface. The health and normal functioning of the ocular surface is dependent on a stable and sufficient tear film. Clinician awareness of conditions affecting the ocular surface has increased in recent years because of expanded research and the publication of diagnosis and treatment guidelines pertaining to disorders resulting in DTS, including the Delphi panel treatment recommendations for DTS (2006), the International Dry Eye Workshop (DEWS) (2007), the Meibomian Gland Dysfunction (MGD) Workshop (2011), and the updated Preferred Practice Pattern guidelines from the American Academy of Ophthalmology pertaining to dry eye and blepharitis (2013). Since the publication of the existing guidelines, new diagnostic techniques and treatment options that provide an opportunity for better management of patients have become available. Clinicians are now able to access a wealth of information that can help them obtain a differential diagnosis and treatment approach for patients presenting with DTS. This review provides a practical and directed approach to the diagnosis and treatment of patients with DTS, emphasizing treatment that is tailored to the specific disease subtype as well as the severity of the condition.
Figures
References
-
- Behrens A, Doyle JJ, Stern L, et al. Dysfunctional Tear Syndrome Study Group Dysfunctional tear syndrome: a Delphi approach to treatment recommendations. Cornea 2006; 25:900–907. - PubMed
-
- Begley CG, Chalmers RL, Abetz L, et al. The relationship between habitual patient-reported symptoms and clinical signs among patients with dry eye of varying severity. Invest Ophthalmol Vis Sci 2003; 44:4753–4761. - PubMed
-
- Nichols KK, Nichols JJ, Mitchell GL. The lack of association between signs and symptoms in patients with dry eye disease. Cornea 2004; 23:762–770. - PubMed
-
- Fiscella RG. Understanding dry eye disease: a managed care perspective. Am J Manag Care 2011; 17:S432–S439. - PubMed
-
- Donnenfeld ED, Solomon R, Roberts CW, et al. Cyclosporine 0.05% to improve visual outcomes after multifocal intraocular lens implantation. J Cataract Refract Surg 2010; 36:1095–1100. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
