

PNEUMATIC VITREOLYSIS FOR RELIEF OF VITREOMACULAR TRACTION
- PMID: 28099316
- PMCID: PMC5642323
- DOI: 10.1097/IAE.0000000000001448
PNEUMATIC VITREOLYSIS FOR RELIEF OF VITREOMACULAR TRACTION
Abstract
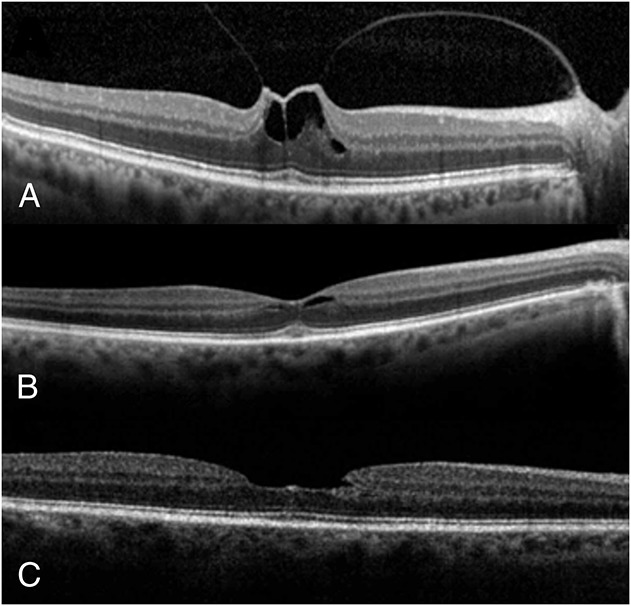
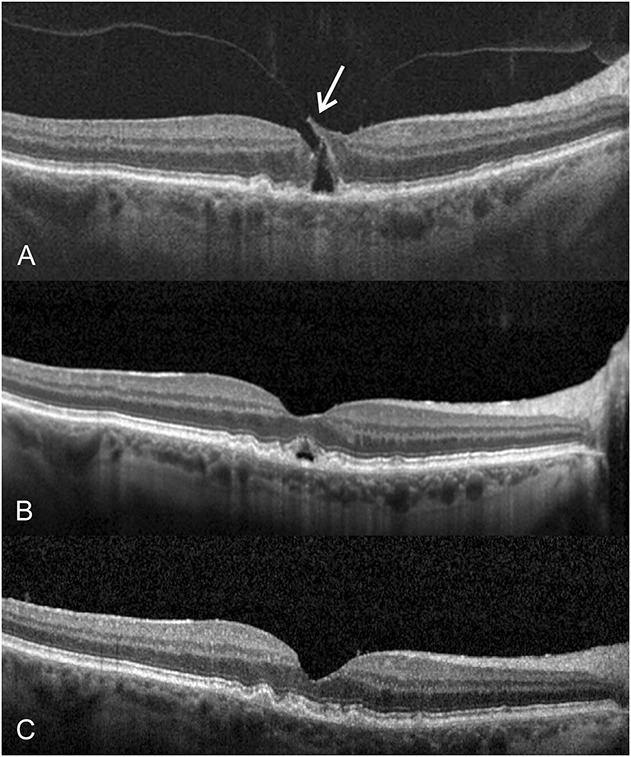
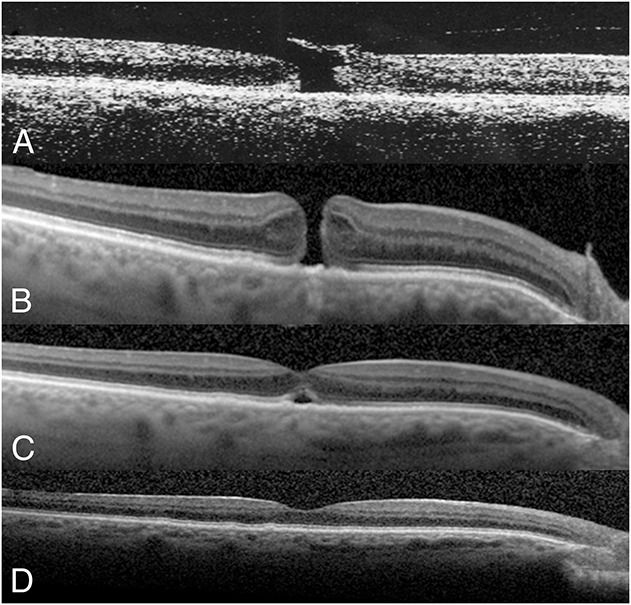
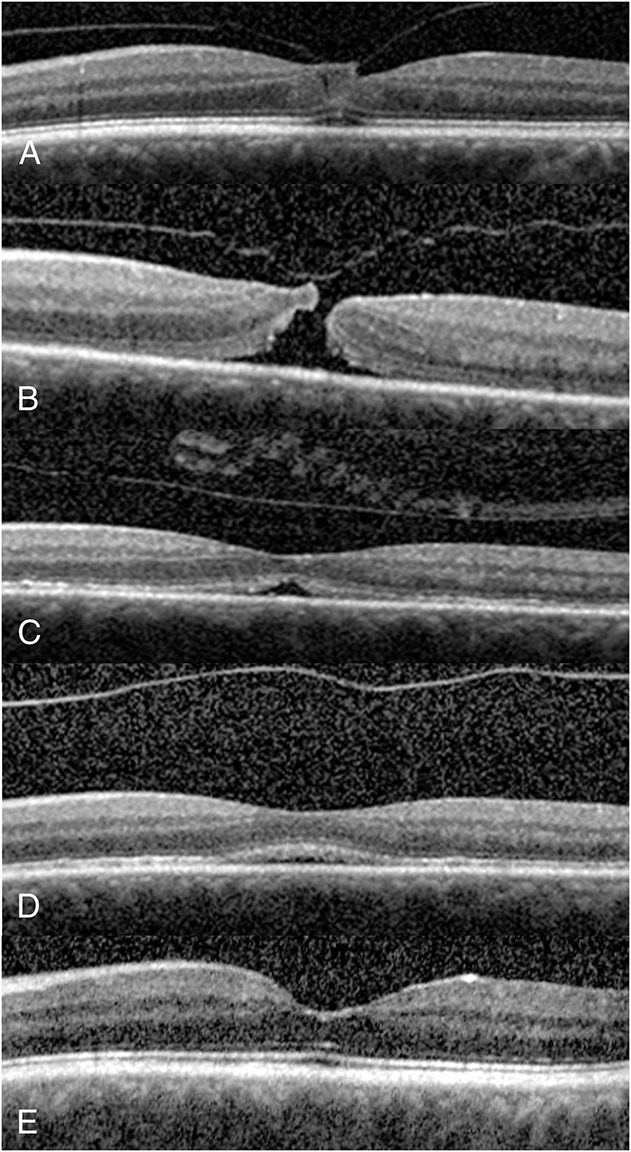
Purpose: To evaluate the outcome of perfluoropropane (C3F8) gas injection for symptomatic vitreomacular traction (VMT) with or without Stage 2 macular hole (MH).
Methods: A retrospective review of eyes with VMT treated with 0.3 mL of C3F8 gas was performed. Patients avoided the supine position until gas resolution. Patients with small MH maintained partial face-down positioning.
Results: Forty-nine consecutive patients (50 eyes) with symptomatic VMT underwent pneumatic vitreolysis between 2010 and 2016. A posterior vitreous detachment developed in 43 eyes (86.0%) after a single gas injection, at a median of 3.0 weeks. Twenty-eight of 35 eyes (80.0%) with VMT only and all 15 eyes (100%) with a small Stage 2 MH developed a posterior vitreous detachment, with MH closure in 10 of 15 eyes (66.7%). Median baseline and last best spectacle-corrected visual acuities were 20/50 and 20/40, respectively (P < 0.001). Mean follow-up time was 11.1 ± 9.9 months. Rate of posterior vitreous detachment was reduced with presence of diabetes mellitus (25%) and with thick cellophane membrane (50%). Univariate analysis showed increased VMT release for eyes with VMT extent within 1 disk area (χ = 13.1, P = 0.002), eyes with absence of diabetes mellitus (χ = 8.8, P = 0.007), and eyes with Stage 2 MH (χ = 5.47, P = 0.019); there was a trend between success and lack of thick cellophane membrane (χ = 3.32, P = 0.068). Results using logistic regression also showed younger age (P = 0.012), followed by better baseline best spectacle-corrected visual acuity (P = 0.044), lack of diabetes mellitus (P = 0.077), and female gender (P = 0.045) to be predictors of increased VMT release. One VMT-only eye formed a MH and another VMT-only eye developed a retinal detachment. Both eyes responded to vitrectomy.
Conclusion: Pneumatic vitreolysis with limited face-down position is a viable option for treating VMT with few adverse events. More studies are needed to elucidate its indications, benefits, and risks.
Conflict of interest statement
None of the authors have any financial/conflicting interests to disclose.
Figures
References
-
- Sebag J. Is pharmacologic vitreolysis brewing? Retina 2002;22:1–3. - PubMed
-
- Sebag J. Pharmacologic vitreolysis, premise and promise of the first decade. Retina 2009;29:871–874. - PubMed
-
- Duker JS, Kaiser PK, Binder S, et al. The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology 2013;120:2611–2619. - PubMed
-
- Hikichi T, Yoshida A, Trempe CL. Course of vitreomacular traction syndrome. Am J Ophthalmol 1995;119:55–61. - PubMed
-
- Sulkes DJ, Ip MS, Baumal CR, et al. Spontaneous resolution of vitreomacular traction documented by optical coherence tomography. Arch Ophthalmol 2000;118:286–287. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
