

Vitamin D insufficiency in neonatal hypoxic-ischemic encephalopathy
- PMID: 28099429
- PMCID: PMC5509506
- DOI: 10.1038/pr.2017.13
Vitamin D insufficiency in neonatal hypoxic-ischemic encephalopathy
Abstract
Background: Vitamin D has neuroprotective and immunomodulatory properties, and deficiency is associated with worse stroke outcomes. Little is known about effects of hypoxia-ischemia or hypothermia treatment on vitamin D status in neonates with hypoxic-ischemic encephalopathy (HIE). We hypothesized vitamin D metabolism would be dysregulated in neonatal HIE altering specific cytokines involved in Th17 activation, which might be mitigated by hypothermia.
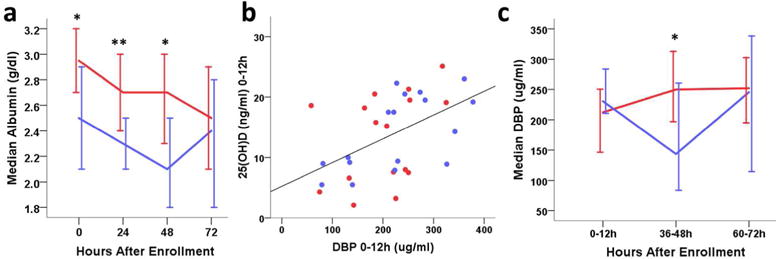
Methods: We analyzed short-term relationships between 25(OH) and 1,25(OH)2 vitamin D, vitamin D binding protein, and cytokines related to Th17 function in serum samples from a multicenter randomized controlled trial of hypothermia 33 °C for 48 h after HIE birth vs. normothermia in 50 infants with moderate to severe HIE.
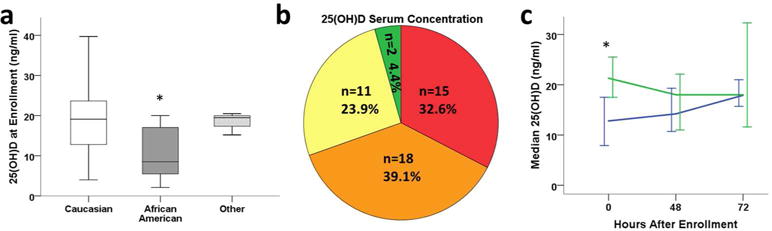
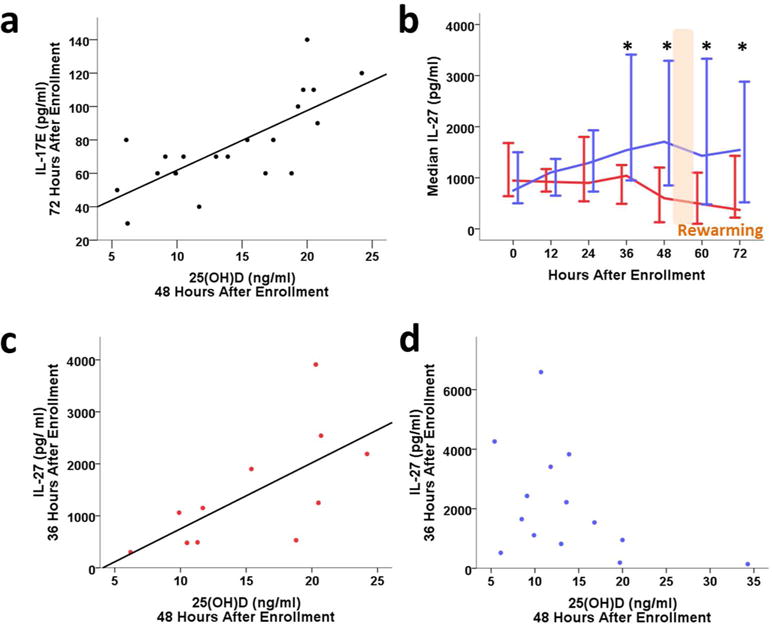
Results: Insufficiency of 25(OH) vitamin D was observed after birth in 70% of infants, with further decline over the first 72 h, regardless of treatment. 25(OH) vitamin D positively correlated with anti-inflammatory cytokine IL-17E in all HIE infants. However, Th17 cytokine suppressor IL-27 was significantly increased by hypothermia, negating the IL-27 correlation with vitamin D observed in normothermic HIE infants.
Conclusion: Serum 25(OH) vitamin D insufficiency is present in the majority of term HIE neonates and is related to lower circulating anti-inflammatory IL-17E. Hypothermia does not mitigate vitamin D deficiency in HIE.
Figures
References
-
- Daumas A, Daubail B, Legris N, et al. Association between Admission Serum 25-Hydroxyvitamin D Levels and Functional Outcome of Thrombolyzed Stroke Patients. J Stroke Cerebrovasc Dis. 2016;25:907–913. - PubMed
-
- Park KY, Chung PW, Kim YB, et al. Serum Vitamin D Status as a Predictor of Prognosis in Patients with Acute Ischemic Stroke. Cerebrovasc Dis. 2015;40:73–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
