

Clinical and pathological characteristics of HIV- and HHV-8-negative Castleman disease
- PMID: 28100459
- PMCID: PMC5364343
- DOI: 10.1182/blood-2016-11-748855
Clinical and pathological characteristics of HIV- and HHV-8-negative Castleman disease
Abstract
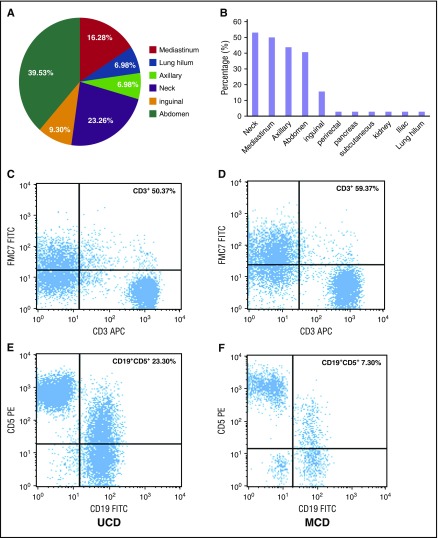
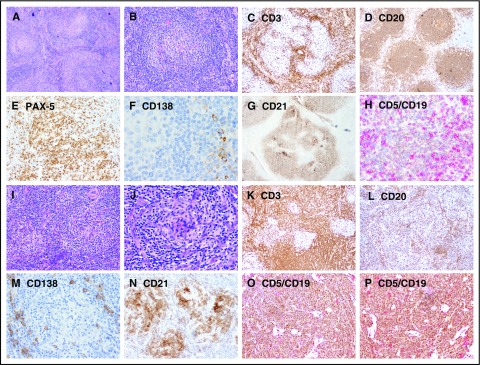
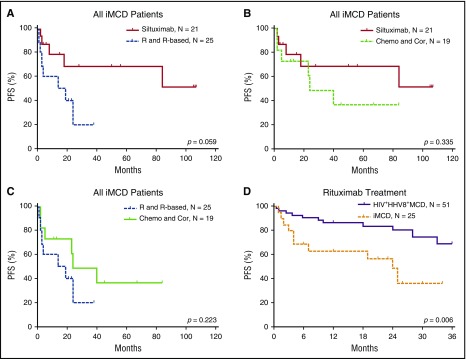
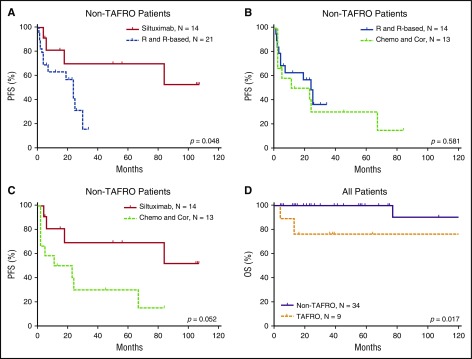
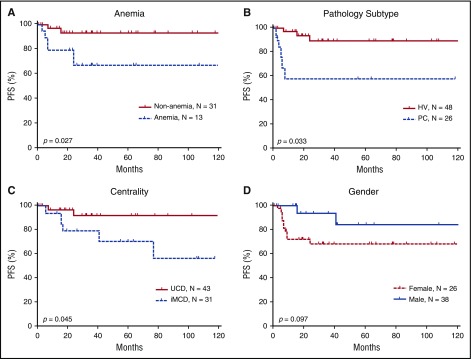
Castleman disease (CD) comprises 3 poorly understood lymphoproliferative variants sharing several common histopathological features. Unicentric CD (UCD) is localized to a single region of lymph nodes. Multicentric CD (MCD) manifests with systemic inflammatory symptoms and organ dysfunction due to cytokine dysregulation and involves multiple lymph node regions. Human herpesvirus 8 (HHV-8) causes MCD (HHV-8-associated MCD) in immunocompromised individuals, such as HIV-infected patients. However, >50% of MCD cases are HIV and HHV-8 negative (defined as idiopathic [iMCD]). The clinical and biological behavior of CD remains poorly elucidated. Here, we analyzed the clinicopathologic features of 74 patients (43 with UCD and 31 with iMCD) and therapeutic response of 96 patients (43 with UCD and 53 with iMCD) with HIV-/HHV-8-negative CD compared with 51 HIV-/HHV-8-positive patients. Systemic inflammatory symptoms and elevated inflammatory factors were more common in iMCD patients than UCD patients. Abnormal bone marrow features were more frequent in iMCD (77.0%) than UCD (45%); the most frequent was plasmacytosis, which was seen in 3% to 30.4% of marrow cells. In the lymph nodes, higher numbers of CD3+ lymphocytes (median, 58.88 ± 20.57) and lower frequency of CD19+/CD5+ (median, 5.88 ± 6.52) were observed in iMCD patients compared with UCD patients (median CD3+ cells, 43.19 ± 17.37; median CD19+/CD5+ cells, 17.37 ± 15.80). Complete surgical resection is a better option for patients with UCD. Siltuximab had a greater proportion of complete responses and longer progression-free survival (PFS) for iMCD than rituximab. Centricity, histopathological type, and anemia significantly impacted PFS. This study reveals that CD represents a heterogeneous group of diseases with differential immunophenotypic profiling and treatment response.
Figures
Comment in
-
Unraveling Castleman: progress in a complex process.Blood. 2017 Mar 23;129(12):1570. doi: 10.1182/blood-2017-02-764654. Blood. 2017. PMID: 28336728 Free PMC article.
References
-
- Fajgenbaum DC, van Rhee F, Nabel CS. HHV-8-negative, idiopathic multicentric Castleman disease: novel insights into biology, pathogenesis, and therapy. Blood. 2014;123(19):2924-2933. - PubMed
-
- Suda T, Katano H, Delsol G, et al. HHV-8 infection status of AIDS-unrelated and AIDS-associated multicentric Castleman’s disease. Pathol Int. 2001;51(9):671-679. - PubMed
-
- Liu AY, Nabel CS, Finkelman BS, et al. Idiopathic multicentric Castleman’s disease: a systematic literature review. Lancet Haematol. 2016;3(4):e163-e175. - PubMed
-
- Munshi N, Mehra M, van de Velde H, Desai A, Potluri R, Vermeulen J. Use of a claims database to characterize and estimate the incidence rate for Castleman disease. Leuk Lymphoma. 2015;56(5):1252-1260. - PubMed
-
- Soumerai JD, Sohani AR, Abramson JS. Diagnosis and management of Castleman disease. Cancer Contr. 2014;21(4):266-278. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
