

Prevalence of Masked Hypertension Among US Adults With Nonelevated Clinic Blood Pressure
- PMID: 28100465
- PMCID: PMC5860080
- DOI: 10.1093/aje/kww237
Prevalence of Masked Hypertension Among US Adults With Nonelevated Clinic Blood Pressure
Abstract
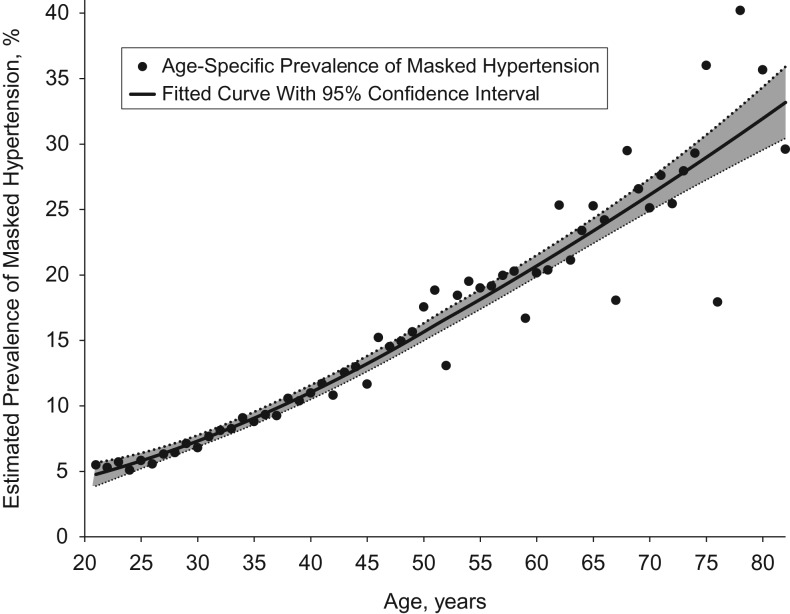
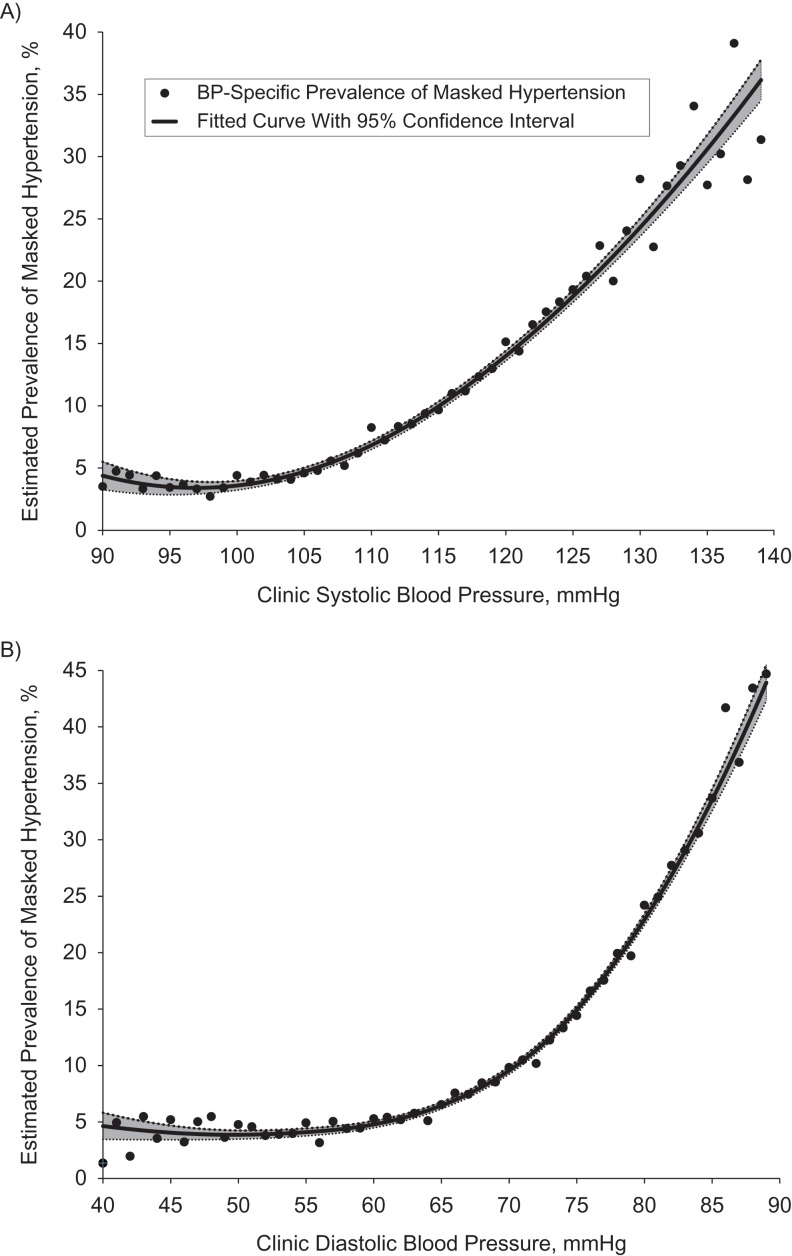
Masked hypertension (MHT), defined as nonelevated blood pressure (BP) in the clinic setting and elevated BP assessed by ambulatory monitoring, is associated with increased risk of target organ damage, cardiovascular disease, and mortality. Currently, no estimate of MHT prevalence exists for the general US population. After pooling data from the Masked Hypertension Study (n = 811), a cross-sectional clinical investigation of systematic differences between clinic BP and ambulatory BP (ABP) in a community sample of employed adults in the New York City metropolitan area (2005-2012), and the National Health and Nutrition Examination Survey (NHANES; 2005-2010; n = 9,316), an ongoing nationally representative US survey, we used multiple imputation to impute ABP-defined hypertension status for NHANES participants and estimate MHT prevalence among the 139 million US adults with nonelevated clinic BP, no history of overt cardiovascular disease, and no use of antihypertensive medication. The estimated US prevalence of MHT in 2005-2010 was 12.3% of the adult population (95% confidence interval: 10.0, 14.5)-approximately 17.1 million persons aged ≥21 years. Consistent with prior research, estimated MHT prevalence was higher among older persons, males, and those with prehypertension or diabetes. To our knowledge, this study provides the first estimate of US MHT prevalence-nearly 1 in 8 adults with nonelevated clinic BP-and suggests that millions of US adults may be misclassified as not having hypertension.
Keywords: ambulatory blood pressure; blood pressure; masked hypertension; multiple imputation; prevalence.
© The Author 2017. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289(19):2560–2572. - PubMed
-
- James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–520. - PubMed
-
- Pickering TG. The ninth Sir George Pickering memorial lecture. Ambulatory monitoring and the definition of hypertension [editorial]. J Hyptertens. 1992;10(5):401–409. - PubMed
-
- Pickering TG, James GD, Boddie C, et al. How common is white coat hypertension. JAMA. 1988;259(2):225–228. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
