

Preventive transarterial embolization in upper nonvariceal gastrointestinal bleeding
- PMID: 28101125
- PMCID: PMC5237324
- DOI: 10.1186/s13017-016-0114-1
Preventive transarterial embolization in upper nonvariceal gastrointestinal bleeding
Abstract
Background: Transarterial embolization (TAE) is a therapeutic option for patients with a high risk of recurrent bleeding after endoscopic haemostasis. The aim of our prospective study was a preliminary assessment of the safety, efficacy, and clinical outcomes following preventive TAE in patients with non-variceal acute upper gastrointestinal bleeding (NVUGIB) with a high risk of recurrent bleeding after endoscopic haemostasis.
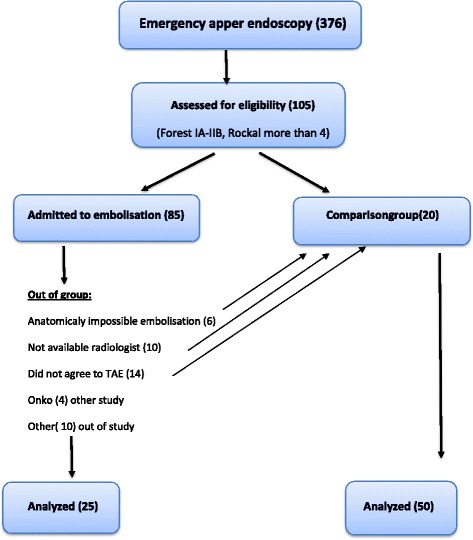
Methods: Preventive visceral angiography and TAE were performed after endoscopic haemostasis on patients with NVUGIB who were at a high risk of recurrent bleeding (PE+ group). The comparison group consisted of similar patients who only underwent endoscopic haemostasis, without preventive TAE (PE- group). The technical success of preventive TAE, the completeness of haemostasis, the incidence of rebleeding and the need for surgical intervention and the main outcomes were compared between the groups.
Results: The PE+ group consisted of 25 patients, and the PE- group of 50 patients, similar in age (median age 66 vs. 63 years), gender and comorbid conditions. The ulcer size at endoscopy was not significantly different (median of 152 mm vs. 127 mm). The most frequent were Forest II type ulcers, 44% in both groups. The distribution of the Forest grade was even. The median haemoglobin on admission was 8, 2 g/dl vs. 8,7 g/dl, p = 0,482, erythrocyte count was 2,7 × 1012/L vs. 2,9 × 1012/L, p = 0,727. The shock index and Rockall scores were similar, as well as and transfusion - on average, four units of packed red blood cells for the majority of patients in both groups, however, significantly more fresh frozen plasma was transfused in the PE- group, p = 0,013. The rebleeding rate was similar, while surgical treatment was needed notably more often in the PE- group, 8% vs. 35% accordingly, p = 0,012. The median ICU stay was 3 days, hospital stay - 6 days vs. 9 days, p = 0.079. The overall mortality reached 20%; in the PE+ group it was 4%, not reaching a statistically significant difference.
Conclusion: Preventive TAE is a feasible, safe and effective minimally invasive type of haemostasis decreasing the risk of repeated bleeding and preparing the patient for the definitive surgical intervention when indicated.
Keywords: Nonvariceal upper gastrointestinal bleeding; Preventive embolization; Transarterial.
References
-
- Loffroy R, Rao P, Ota S, De Lin M, Kwak BK, Geschwind JF. Embolization of acute nonvariceal upper gastrointestinal hemorrhage resistant to endoscopic treatment: results and predictors of recurrent bleeding. Cardiovasc Intervent Radiol. 2010;33:1088–1100. doi: 10.1007/s00270-010-9829-7. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
