

Postocclusive Hyperemia Measured with Laser Doppler Flowmetry and Transcutaneous Oxygen Tension in the Diagnosis of Primary Raynaud's Phenomenon: A Prospective, Controlled Study
- PMID: 28101516
- PMCID: PMC5215461
- DOI: 10.1155/2016/9645705
Postocclusive Hyperemia Measured with Laser Doppler Flowmetry and Transcutaneous Oxygen Tension in the Diagnosis of Primary Raynaud's Phenomenon: A Prospective, Controlled Study
Abstract
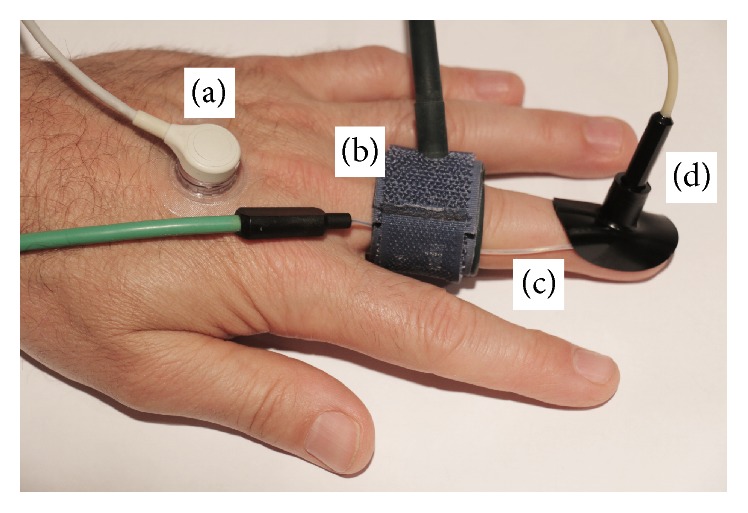
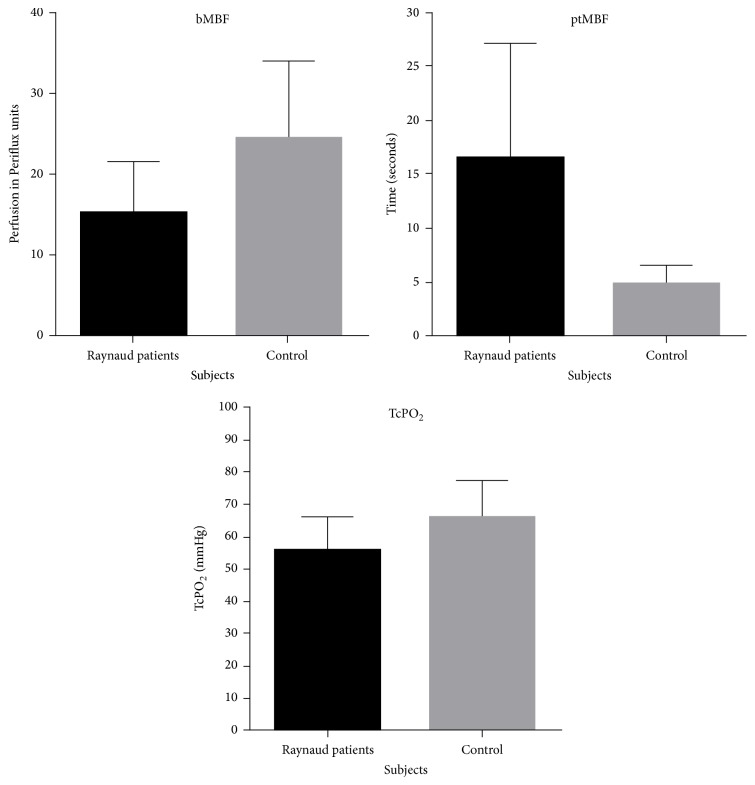
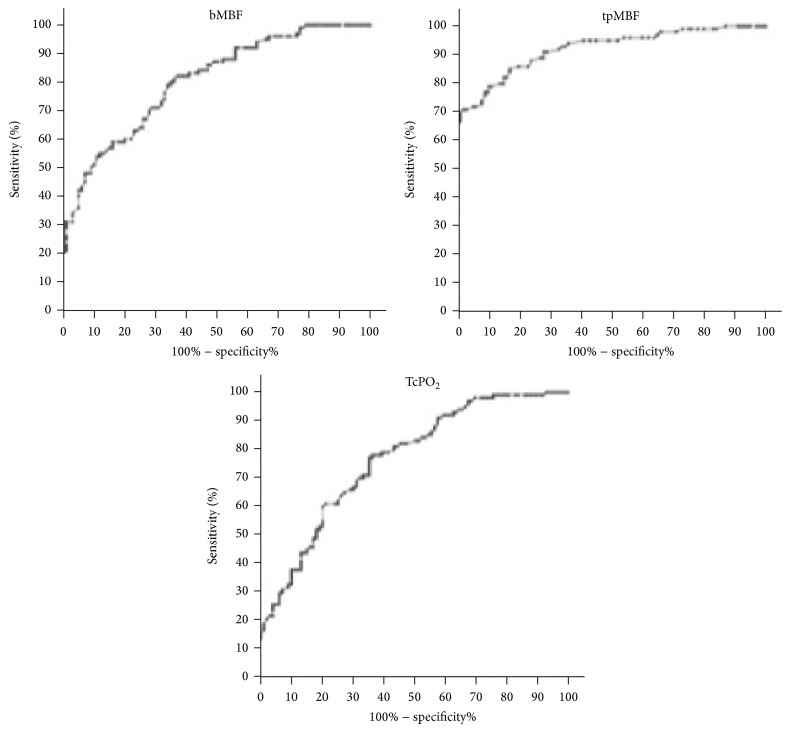
The aim of this study was to measure the sensitivity and specificity of transcutaneous oxygen tension and postocclusive hyperemia testing using laser Doppler flowmetry in patients with primary Raynaud's phenomenon. One hundred patients and one hundred controls were included in the study. Baseline microvascular blood flow and then time to peak flow following occlusion were measured using laser Doppler flowmetry. Afterwards, the transcutaneous oxygen tension was recorded. The sensitivities of baseline microvascular blood flow, postocclusive time to peak flow, and transcutaneous oxygen tension were 79%, 79%, and 77%, respectively. The postocclusive time peak flow had a superior specificity of 90% and area under the curve of 0.92 as compared to 66% and 0.80 for baseline microvascular flow and 64% and 0.76 for transcutaneous oxygen tension. Time to postocclusive peak blood flow measured by laser Doppler flowmetry is a highly accurate test for differentiating patients with primary Raynaud's phenomenon from healthy controls.
Conflict of interest statement
The authors declare that there is no conflict of interests.
Figures
Similar articles
-
Postocclusive reactive hyperemia in hand-arm vibration syndrome.Int J Occup Med Environ Health. 2016;29(4):659-66. doi: 10.13075/ijomeh.1896.00765. Int J Occup Med Environ Health. 2016. PMID: 27443761
-
Abnormal amplitude and kinetics of digital postocclusive reactive hyperemia in systemic sclerosis.Microvasc Res. 2014 Jul;94:90-5. doi: 10.1016/j.mvr.2014.05.007. Epub 2014 Jun 2. Microvasc Res. 2014. PMID: 24990822 Clinical Trial.
-
Postocclusive reactive hyperemia inversely correlates with urinary 15-F2t-isoprostane levels in systemic sclerosis.Free Radic Biol Med. 2006 May 15;40(10):1732-7. doi: 10.1016/j.freeradbiomed.2006.01.014. Epub 2006 Feb 7. Free Radic Biol Med. 2006. PMID: 16678012
-
Cold extremities: investigation and management of Raynaud's phenomenon.J South Orthop Assoc. 1996 Spring;5(1):37-45. J South Orthop Assoc. 1996. PMID: 8673588 Review.
-
Evaluation of microvascular reactivity with laser Doppler flowmetry in chronic kidney disease.World J Nephrol. 2013 Aug 6;2(3):77-83. doi: 10.5527/wjn.v2.i3.77. World J Nephrol. 2013. PMID: 24255889 Free PMC article. Review.
Cited by
-
Raynaud's Phenomenon with Focus on Systemic Sclerosis.J Clin Med. 2022 Apr 28;11(9):2490. doi: 10.3390/jcm11092490. J Clin Med. 2022. PMID: 35566614 Free PMC article. Review.
-
New perspectives in the imaging of Raynaud's phenomenon.Eur J Rheumatol. 2020 Oct;7(Suppl 3):S212-S221. doi: 10.5152/eurjrheum.2020.19124. Epub 2020 Jul 6. Eur J Rheumatol. 2020. PMID: 33164735 Free PMC article. Review.
-
Analysis of Hand Function, Upper Limb Disability, and Its Relationship with Peripheral Vascular Alterations in Raynaud's Phenomenon.Diagnostics (Basel). 2023 Dec 30;14(1):93. doi: 10.3390/diagnostics14010093. Diagnostics (Basel). 2023. PMID: 38201402 Free PMC article.
-
Microvascular dysfunction in ankylosing spondylitis is associated with disease activity and is improved by anti-TNF treatment.Sci Rep. 2018 Sep 4;8(1):13205. doi: 10.1038/s41598-018-31550-y. Sci Rep. 2018. PMID: 30181568 Free PMC article.
References
-
- Raynaud M. On Local Asphyxia and Symmetrical Gangrene of the Extremities. Paris, France: E.Leclerc Paris; 1862.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
