

Risk of arrhythmic death in ischemic heart disease: a prospective, controlled, observer-blind risk stratification over 10 years
- PMID: 28102901
- PMCID: PMC5392777
- DOI: 10.1111/eci.12729
Risk of arrhythmic death in ischemic heart disease: a prospective, controlled, observer-blind risk stratification over 10 years
Abstract
Background: Risk of arrhythmic death is considered highest in ischemic heart disease with severe left ventricular ejection fraction (LVEF) reduction. Non-invasive testing should improve decision-making of prophylactic defibrillator (ICD) implantation.
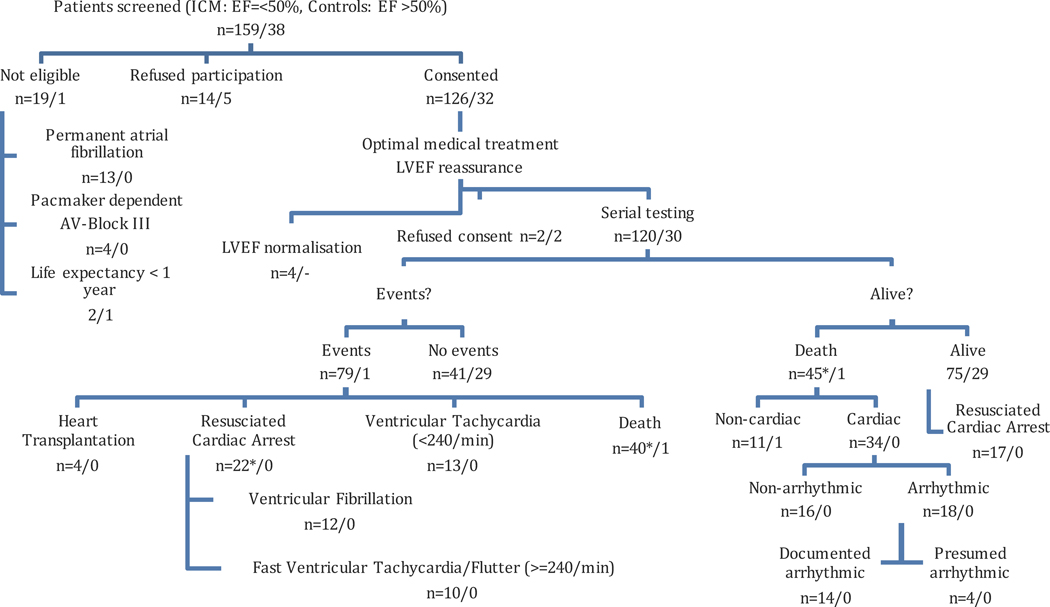
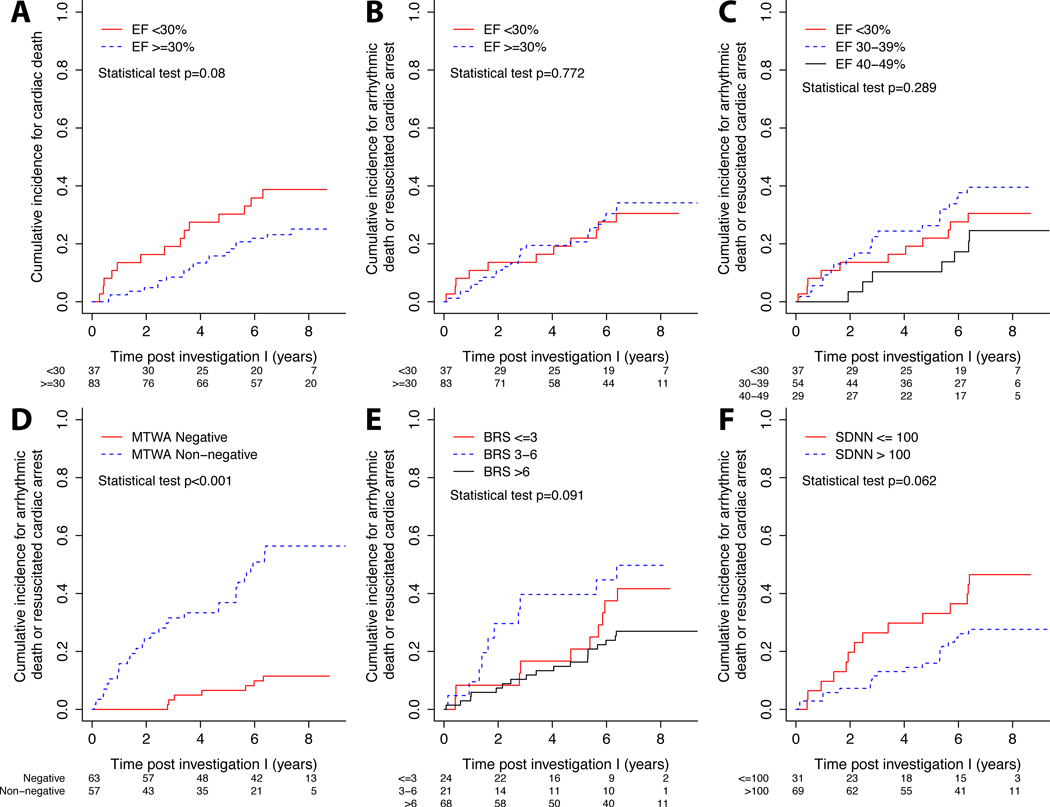
Design: We enrolled 120 patients with ischemic heart disease and LVEF < 50% and 30 control subjects without ischemic heart disease and normal LVEF. An initial assessment, a second assessment after 3 years and a final follow-up comprised of pharmacological baroreflex testing (BRS), short-term spectral [low-frequency (LF) to high-frequency (HF) ratio] and long-term time-domain analysis of heart rate variability (SDNN), exercise Microvolt T-wave alternans (MTWA) and others.
Results: The median follow-up was 7·5 years. Resuscitated cardiac arrest and arrhythmic death due to ventricular arrhythmias ≥ 240/min was observed in 18% and 15% of patients, respectively. Cardiac death was observed in 28% of patients. The incidence of arrhythmic death and resuscitated cardiac arrest was identical in patients with ischemic heart disease with LVEF < 30% and ≥ 30%. No significant difference between subgroups with LVEF of < 30%, 30-39% and ≥ 40% was found either. MTWA, BRS, SDNN and LF to HF ratio failed to identify patients at risk of arrhythmic death in a multiple regression model.
Conclusions: Ischemic heart disease patients with LVEF < 30% and ≥ 30% face the same risk of arrhythmic death. Stratification techniques fail to identify high-risk patients. Therefore, the current practice to constrain prophylactic ICDs to patients with severely reduced LVEF seems to be insufficient.
Keywords: Ischemic heart disease; non-invasive risk stratification; sudden cardiac death.
© 2017 Stichting European Society for Clinical Investigation Journal Foundation.
Conflict of interest statement
For all authors: There is no conflict of interest.
Figures
References
-
- Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators. N Engl J Med. 1996 Dec 26;335(26):1933–1940. - PubMed
-
- Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease. Multicenter Unsustained Tachycardia Trial Investigators. N Engl J Med. 1999 Dec 16;341(25):1882–1890. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002 Mar 21;346(12):877–883. - PubMed
-
- La Rovere MT, Bigger JT, Jr, Marcus FI, Mortara A, Schwartz PJ. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) Investigators. Lancet. 1998 Feb 14;351(9101):478–484. - PubMed
-
- Bloomfield DM, Steinman RC, Namerow PB, et al. Microvolt T-wave alternans distinguishes between patients likely and patients not likely to benefit from implanted cardiac defibrillator therapy: a solution to the Multicenter Automatic Defibrillator Implantation Trial (MADIT) II conundrum. Circulation. 2004 Oct 5;110(14):1885–1889. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
