

Cost-Effectiveness Analysis of Five Competing Strategies for the Management of Multiple Recurrent Community-Onset Clostridium difficile Infection in France
- PMID: 28103289
- PMCID: PMC5245822
- DOI: 10.1371/journal.pone.0170258
Cost-Effectiveness Analysis of Five Competing Strategies for the Management of Multiple Recurrent Community-Onset Clostridium difficile Infection in France
Abstract
Background: Clostridium difficile infection (CDI) is characterized by high rates of recurrence, resulting in substantial health care costs. The aim of this study was to analyze the cost-effectiveness of treatments for the management of second recurrence of community-onset CDI in France.
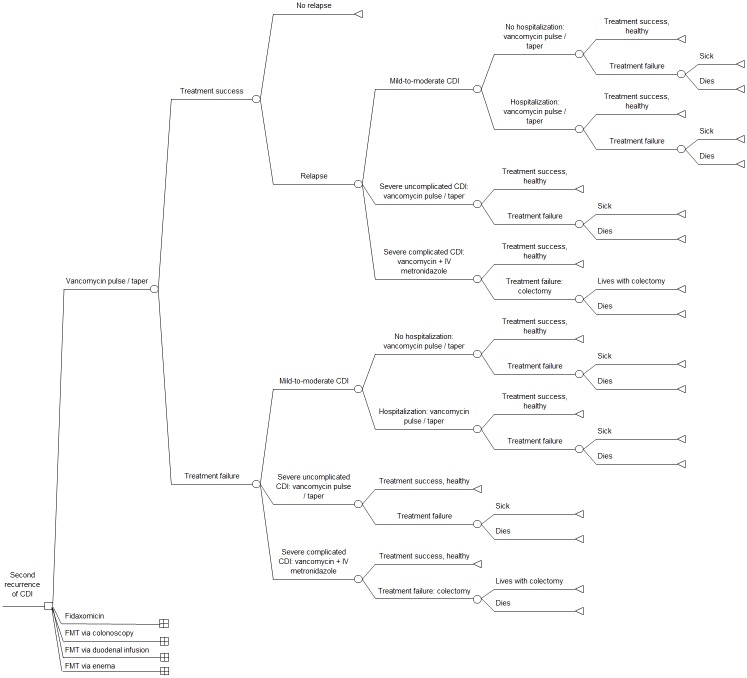
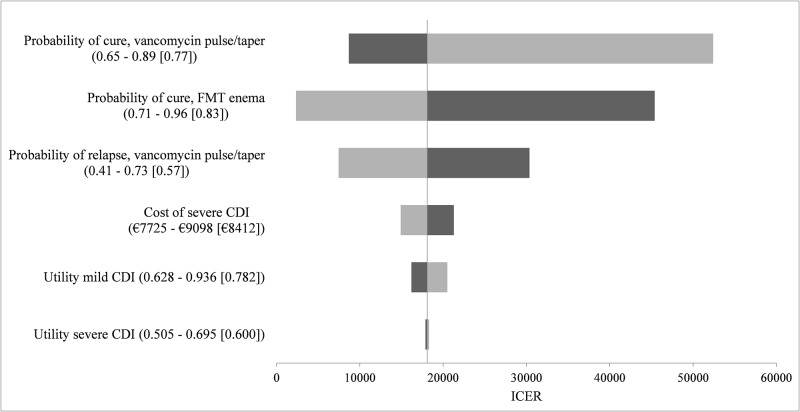
Methods: We developed a decision-analytic simulation model to compare 5 treatments for the management of second recurrence of community-onset CDI: pulsed-tapered vancomycin, fidaxomicin, fecal microbiota transplantation (FMT) via colonoscopy, FMT via duodenal infusion, and FMT via enema. The model outcome was the incremental cost-effectiveness ratio (ICER), expressed as cost per quality-adjusted life year (QALY) among the 5 treatments. ICERs were interpreted using a willingness-to-pay threshold of €32,000/QALY. Uncertainty was evaluated through deterministic and probabilistic sensitivity analyses.
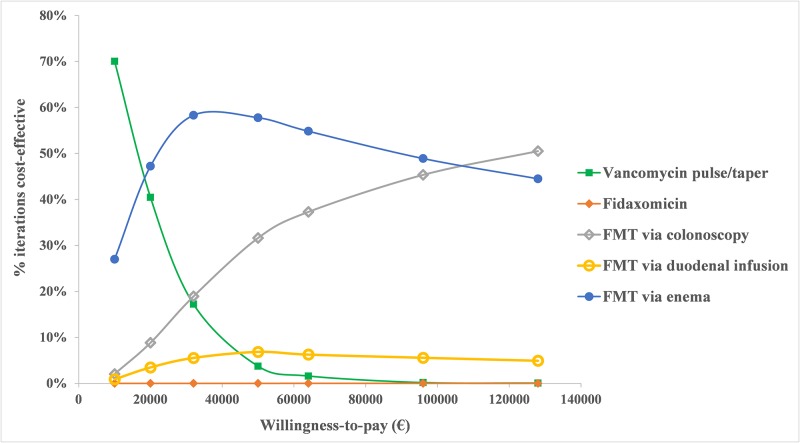
Results: Three strategies were on the efficiency frontier: pulsed-tapered vancomycin, FMT via enema, and FMT via colonoscopy, in order of increasing effectiveness. FMT via duodenal infusion and fidaxomicin were dominated (i.e. less effective and costlier) by FMT via colonoscopy and FMT via enema. FMT via enema compared with pulsed-tapered vancomycin had an ICER of €18,092/QALY. The ICER for FMT via colonoscopy versus FMT via enema was €73,653/QALY. Probabilistic sensitivity analysis with 10,000 Monte Carlo simulations showed that FMT via enema was the most cost-effective strategy in 58% of simulations and FMT via colonoscopy was favored in 19% at a willingness-to-pay threshold of €32,000/QALY.
Conclusions: FMT via enema is the most cost-effective initial strategy for the management of second recurrence of community-onset CDI at a willingness-to-pay threshold of €32,000/QALY.
Conflict of interest statement
The authors of this manuscript have read the journal's policy and have the following competing interests: TG reports personal fees from Astellas and MSD, outside the submitted work. All authors report no competing interests relevant to this article. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Eyre DW, Tracey L, Elliott B, Slimings C, Huntington PG, Stuart RL, et al. Emergence and spread of predominantly community-onset Clostridium difficile PCR ribotype 244 infection in Australia, 2010 to 2012. Euro Surveill. 2015;20(10):21059 - PubMed
-
- Kelly CP. Can we identify patients at high risk of recurrent Clostridium difficile infection? Clin Microbiol Infect. 2012. December;18 Suppl 6:21–7. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
