

Thoracoscopic surgery in the prone position for esophageal cancer in patients with situs inversus totalis: A report of two cases
- PMID: 28103500
- PMCID: PMC5241577
- DOI: 10.1016/j.ijscr.2017.01.009
Thoracoscopic surgery in the prone position for esophageal cancer in patients with situs inversus totalis: A report of two cases
Abstract
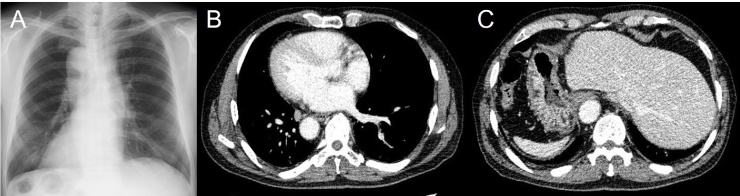
Introduction: Situs inversus totalis (SIT) is a rare congenital condition characterized by a complete transposition of thoracic and abdominal organs. Here, we present two successful cases of left thoracoscopic esophagectomy in the prone position for SIT-associated esophageal cancer.
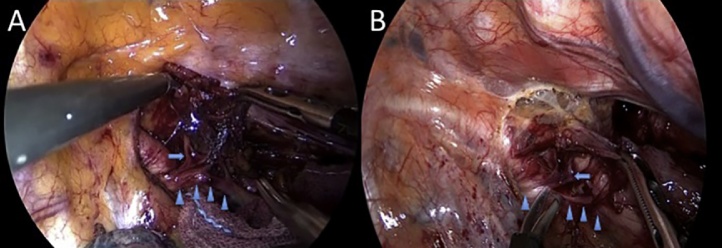
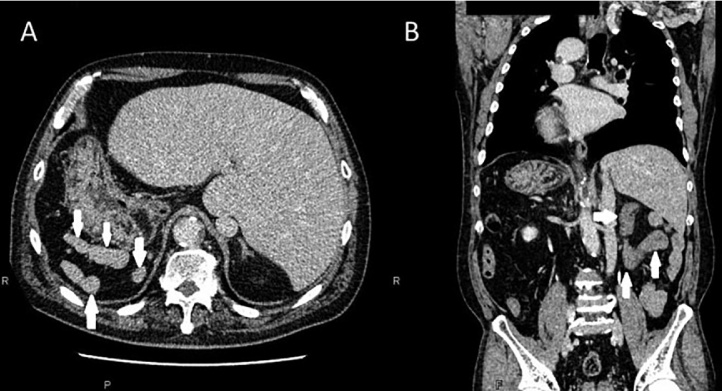
Presentation of case: Our first case was of an 82-year-old man who underwent a left thoracoscopic esophagectomy in the prone position, followed by hand-assisted laparoscopic gastric mobilization. Surgical duration and blood loss were 661min and 165g, respectively. His postoperative course was uneventful. The second case was of a 66-year-old man who underwent a left thoracoscopic esophagectomy in the prone position, followed by gastric mobilization via laparotomy owing to a concomitant intestinal malrotation and polysplenia. Surgical duration and blood loss were 637min and 220g, respectively. We trained for the surgical procedures preoperatively using left-inverted and right-inverted thoracoscopic surgical videos of patients with normal anatomy.
Discussion: Surgical procedures in SIT patients are challenging owing to their mirrored anatomy. Recognition of their variations is thus important to avoid intraoperative accidental injuries. Left-inverted and right-inverted thoracoscopic surgical videos of patients with normal anatomy were found to be useful for image training prior to the actual surgery.
Conclusion: Thoracoscopic surgical treatment for esophageal cancer associated with SIT in the prone position can be performed safely, similar to the manner performed for thoracoscopic surgery in the right decubitus position, or surgery via an open thoracotomy. Gastric mobilization via laparotomy should be considered in patients associated other anatomic variations.
Keywords: Intestinal malrotation; Laparoscopy; Polysplenia; Thoracoscopy; Video.
Copyright © 2017 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Yagi Y., Yoshimitsu Y., Maeda T., Sakuma H., Watanabe M., Nakai M. Thoracoscopic esophagectomy and hand-assisted laparoscopic gastric mobilization for esophageal cancer with situs inversus totalis. J. Gastrointest. Surg. 2012;16:1235–1239. [PMID. 22125175] - PubMed
-
- Peel J., Darling G. Left video-assisted thoracoscopic surgery esophagectomy in a patient with situs inversus totalis and Kartagener syndrome. Ann. Thorac. Surg. 2014;98:706–708. [PMID. 25087796] - PubMed
-
- Yoshida T., Usui S., Inoue H., Kudo S.E. The management of esophageal cancer with situs inversus totalis by simultaneous hand-assisted laparoscopic gastric mobilization and thoracoscopic esophagectomy. J. Laparoendosc. Adv. Surg. Technol. A. 2004;14:384–389. [PMID. 15684787] - PubMed
-
- Ujiie N., Nakano T., Kamei T., Ichikawa H., Miyata G., Onodera K. Thoracoscopic esophagectomy for esophageal cancer with situs inversus totalis: a case report and literature review. Gen. Thorac. Cardiovasc. Surg. 2016;64:359–362. [PMID. 26984287] - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
