

The Experience of Hospital Death: Assessing the Quality of Care at an Academic Medical Center
- PMID: 28103711
- PMCID: PMC5711599
- DOI: 10.1177/1049909116689547
The Experience of Hospital Death: Assessing the Quality of Care at an Academic Medical Center
Abstract
Background: The quality of perimortem care received by patients who died at our hospitals was unknown.
Objective: To describe the quality of hospital care experienced in the last week of life, as perceived by decedents' families.
Design: Telephone survey that included established measures and investigator-developed content.
Setting: Large, tertiary care center known for high-quality, cost-effective care.
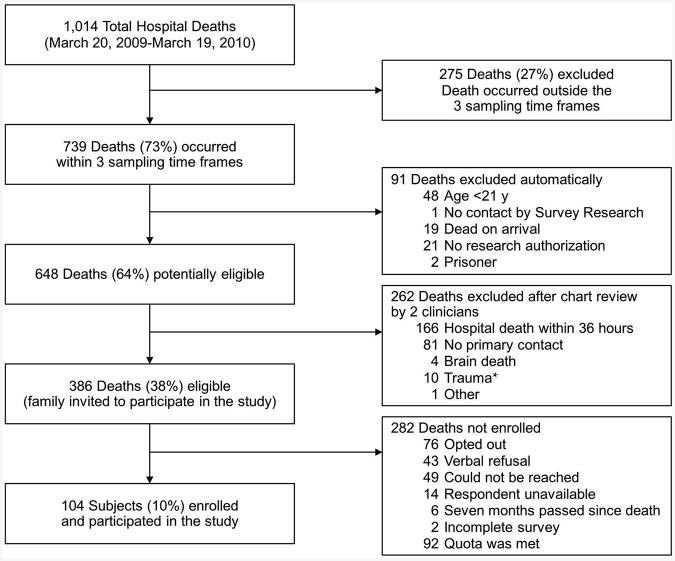
Participants: Family members of 104 patients who died in-hospital (10% of annual deaths) over the course of 1 year.
Intervention: None.
Measurements: Participant perceptions of the decedent's care, including symptom management, personal care, communication, and care coordination.
Results: Decedents were mostly male (64%), white (96%), married (73%), and Christian (91%). Most survey participants were spouses of the decedent (68%); they were predominately white (98%), female (70%), and Christian (90%) and had a median age of 70 years (range, 35-91 years). Overall satisfaction was high. Pain, dyspnea, and anxiety or sadness were highly prevalent among decedents (73%, 73%, and 55%, respectively) but largely well managed. Most participants believed that decedents were treated respectfully and kindly by staff (87%) and that sufficient help was available to assist with medications and dressing changes (97%). Opportunities for improvement included management of decedents' anxiety or sadness (29%) and personal care (25%), emotional support of the family (57%), communication regarding decedents' illness (29%), and receiving contradictory or confusing information (33%).
Conclusion: Despite high satisfaction with care overall, we identified important unmet needs. Addressing these gaps will improve the care of dying patients.
Keywords: death; decedent; family caregivers; hospitals; quality of health care; terminal care.
Conflict of interest statement
Conflict of interest: None.
Figures
Similar articles
-
Out-of-hospital death: advance care planning, decedent symptoms, and caregiver burden.J Am Geriatr Soc. 2004 Apr;52(4):532-9. doi: 10.1111/j.1532-5415.2004.52158.x. J Am Geriatr Soc. 2004. PMID: 15066067
-
A pilot study to explore next of kin's perspectives on end-of-life care in the nursing home.J Am Med Dir Assoc. 2011 Feb;12(2):135-42. doi: 10.1016/j.jamda.2010.07.017. Epub 2010 Oct 16. J Am Med Dir Assoc. 2011. PMID: 21266290
-
Symptom experiences of residents dying in assisted living.J Am Med Dir Assoc. 2006 May;7(4):219-23. doi: 10.1016/j.jamda.2005.09.011. Epub 2005 Nov 23. J Am Med Dir Assoc. 2006. PMID: 16698507
-
Systematic Review for the Quality of End-of-Life Care for Patients With Dementia in the Hospital Setting.Am J Hosp Palliat Care. 2018 Dec;35(12):1572-1583. doi: 10.1177/1049909118776985. Epub 2018 Jun 5. Am J Hosp Palliat Care. 2018. PMID: 29871500
-
Dying in the hospital setting: A meta-synthesis identifying the elements of end-of-life care that patients and their families describe as being important.Palliat Med. 2017 Jul;31(7):587-601. doi: 10.1177/0269216316673547. Epub 2016 Dec 8. Palliat Med. 2017. PMID: 27932631 Review.
Cited by
-
Better end-of-life care in surgical patients: Veterans Affairs Bereaved Family Survey - a qualitative analysis.BMJ Support Palliat Care. 2025 Feb 26;15(2):270-280. doi: 10.1136/spcare-2024-004873. BMJ Support Palliat Care. 2025. PMID: 39578044 Free PMC article.
-
Concerns and potential improvements in end-of-life care from the perspectives of older patients and informal caregivers: a scoping review.BMC Geriatr. 2021 Dec 20;21(1):729. doi: 10.1186/s12877-021-02680-2. BMC Geriatr. 2021. PMID: 34930177 Free PMC article.
-
Facilitating family needs and support at the end of life in hospital: A descriptive study.Palliat Med. 2022 Mar;36(3):549-554. doi: 10.1177/02692163211066431. Epub 2021 Dec 30. Palliat Med. 2022. PMID: 34965777 Free PMC article.
-
Trends in End-of-Life Care and Satisfaction Among Veterans Undergoing Surgery.Ann Surg. 2025 Apr 1;281(4):682-688. doi: 10.1097/SLA.0000000000006253. Epub 2024 Feb 23. Ann Surg. 2025. PMID: 38390769
-
Caregiver perceptions of end-of-life care in patients with high-grade glioma.Neurooncol Pract. 2020 Nov 20;8(2):171-178. doi: 10.1093/nop/npaa077. eCollection 2021 Apr. Neurooncol Pract. 2020. PMID: 33898050 Free PMC article.
References
-
- Wennberg JE, Fisher ES, Goodman DC, Skinner JS. In: Tracking the care of patients with severe chronic illness: the Dartmouth Atlas of Health Care 2008. Bronner KK, editor. Lebanon (NH): Dartmouth Medical School; 2008. - PubMed
-
- Hall MJ, Levant S, DeFrances CJ. NCHS Data Brief. 118. 2013. Mar, Trends in inpatient hospital deaths: National Hospital Discharge Survey, 2000-2010; pp. 1–8. - PubMed
-
- Goodman DC, Fisher ES, Wennberg JE, Skinner JS, Chasan-Taber S, Bronner KK. Tracking improvement in the care of chronically ill patients: a Dartmouth Atlas brief on medicare beneficiaries near the end of life. Lebanon (NH): Dartmouth Institute for Health Policy and Clinical Practice: a report of the Dartmouth Atlas Project; 2013. - PubMed
-
- Goodman DC, Esty AR, Fisher ES, Chang CH. In: Trends and variation in end-of-life care for Medicare beneficiaries with severe chronic illness. Bronner KK, editor. Lebanon (NH): Dartmouth Institute for Health Policy and Clinical Practice: a report of the Dartmouth Atlas Project; 2011. - PubMed
-
- Institute of Medicine: of the National Academies. Dying in America: improving quality and honoring individual preferences near the end of life. Washington (DC); The National Academies Press; 2015. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
