

Cystic fibrosis physicians' perspectives on the timing of referral for lung transplant evaluation: a survey of physicians in the United States
- PMID: 28103851
- PMCID: PMC5248524
- DOI: 10.1186/s12890-017-0367-9
Cystic fibrosis physicians' perspectives on the timing of referral for lung transplant evaluation: a survey of physicians in the United States
Abstract
Background: Prior studies reveal that a significant proportion of patients with cystic fibrosis (CF) and advanced lung disease are not referred for lung transplant (LTx) evaluation. We sought to assess expert CF physician perspectives on the timing of LTx referral and investigate their LTx knowledge.
Methods: We developed an online anonymous survey that was distributed by the Cystic Fibrosis Foundation (CFF) to the medical directors of all CFF-accredited care centers in the United States in 2015. The survey addressed only adult patients (≥18 years old) and was sent to 119 adult CF physicians, 86 CFF-affiliated CF physicians (who see adults and children, but have smaller program sizes than adult or pediatric centers), and 127 pediatric CF physicians (who see some adults, but mostly children). The focus of the questions was on CFF-care center characteristics, physician experience and indications/contraindications to referral for LTx evaluation.
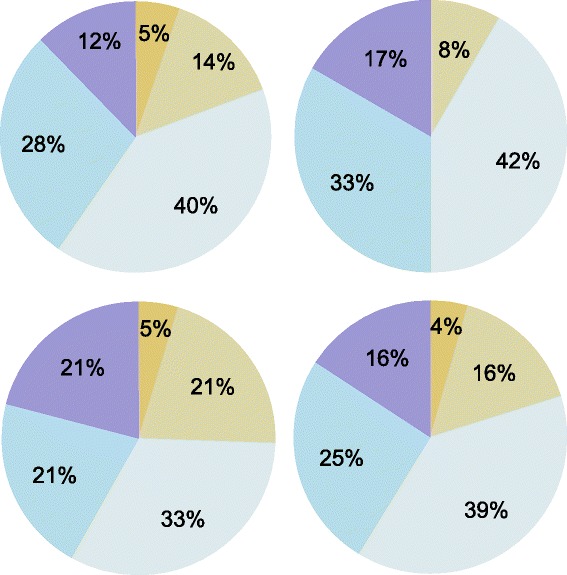
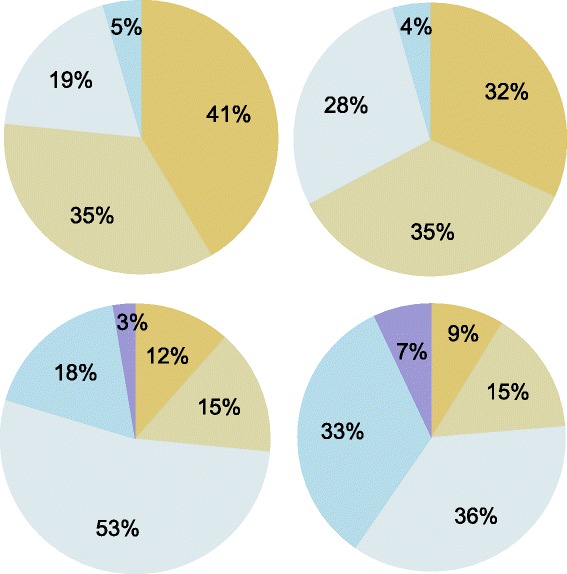
Results: There were 114/332 (34%) total responses to the survey. The response rates were: 57/119 (48%) adult physicians, 12/86 (14%) affiliate physicians and 43/127 (34%) pediatric physicians; 2 physicians did not include their CFF center type. Despite the poor ability of FEV1 < 30% to predict death within 2 years, 94% of responding CF physicians said they would refer an adult patient for LTx evaluation if the patient's lung function fell to FEV1 < 30% predicted. Only 54% of respondents report that pulmonary hypertension would trigger referral. Pulmonary hypertension is an internationally recommended indication to list a patient for LTx (not just for referral for evaluation). Very few physicians (N = 17, 15%) employed components of the lung allocation score (LAS) to determine the timing of referral for LTx evaluation. Interestingly, patient preference not to undergo LTx was "often" or "always" the primary patient-related reason to defer referral for LTx evaluation for 41% (47/114) of respondents.
Conclusions: Some potential barriers to timely LTx referral for patients with CF include physician knowledge regarding non-lung function-based recommendations related to timing of referral and listing for LTx, and patient preference not to undergo LTx. Further exploration of physician-level and CF patient-level barriers to timely LTx referral is warranted.
Keywords: Cystic fibrosis; Lung transplantation; Physician survey; Referral.
Figures


References
-
- Cystic Fibrosis Foundation Patient Registry, 2012 Annual Data Report. Bethesda, Maryland; 2013.
-
- Ramos K, Quon B, Heltshe S, Hamblett N, Aitken M, Goss C. HETEROGENEITY IN SURVIVAL AMONG ADULT CYSTIC FIBROSIS PATIENTS WITH LOW LUNG FUNCTION. 2015 North American Cystic Fibrosis Conference. 111 RIVER ST, HOBOKEN 07030–5774, NJ USA: WILEY-BLACKWELL; 2015. p. 350.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
