

The interaction between vaginal microbiota, cervical length, and vaginal progesterone treatment for preterm birth risk
- PMID: 28103952
- PMCID: PMC5244550
- DOI: 10.1186/s40168-016-0223-9
The interaction between vaginal microbiota, cervical length, and vaginal progesterone treatment for preterm birth risk
Abstract
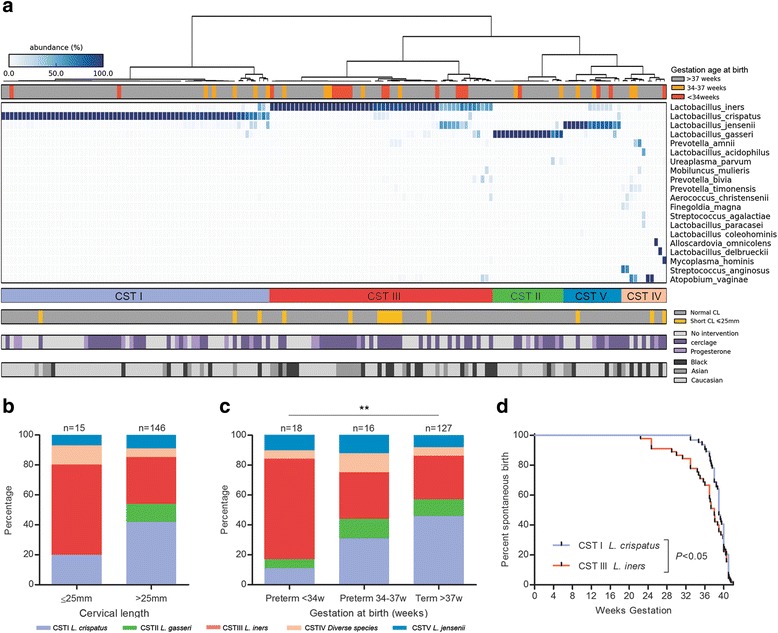
Background: Preterm birth is the primary cause of infant death worldwide. A short cervix in the second trimester of pregnancy is a risk factor for preterm birth. In specific patient cohorts, vaginal progesterone reduces this risk. Using 16S rRNA gene sequencing, we undertook a prospective study in women at risk of preterm birth (n = 161) to assess (1) the relationship between vaginal microbiota and cervical length in the second trimester and preterm birth risk and (2) the impact of vaginal progesterone on vaginal bacterial communities in women with a short cervix.
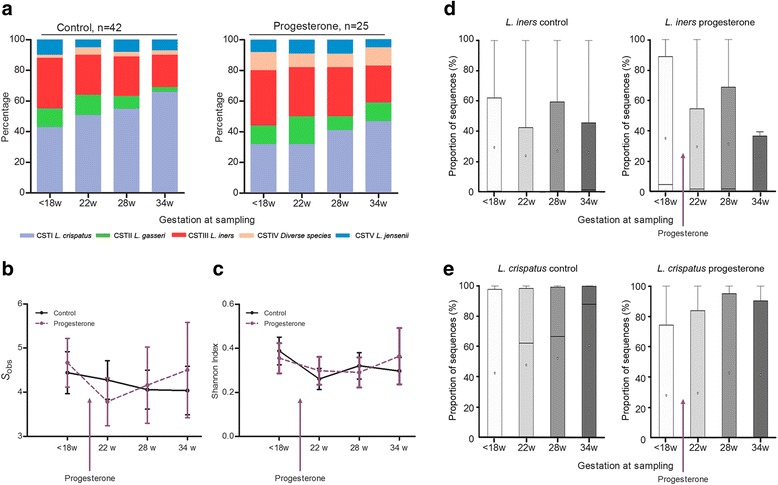
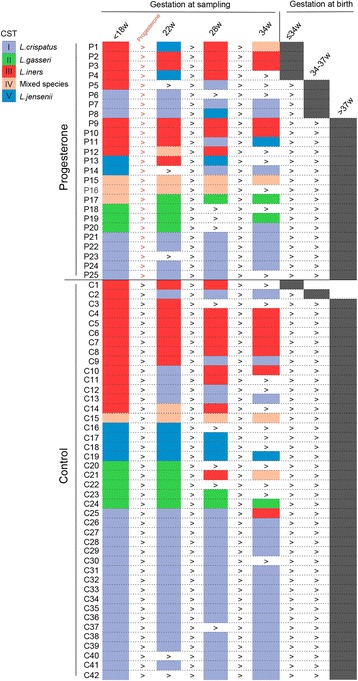
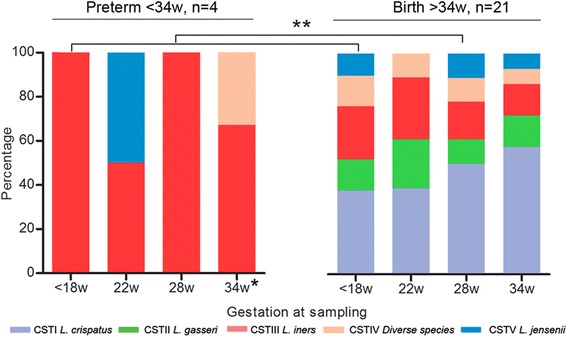
Results: Lactobacillus iners dominance at 16 weeks of gestation was significantly associated with both a short cervix <25 mm (n = 15, P < 0.05) and preterm birth <34+0 weeks (n = 18; P < 0.01; 69% PPV). In contrast, Lactobacillus crispatus dominance was highly predictive of term birth (n = 127, 98% PPV). Cervical shortening and preterm birth were not associated with vaginal dysbiosis. A longitudinal characterization of vaginal microbiota (<18, 22, 28, and 34 weeks) was then undertaken in women receiving vaginal progesterone (400 mg/OD, n = 25) versus controls (n = 42). Progesterone did not alter vaginal bacterial community structure nor reduce L. iners-associated preterm birth (<34 weeks).
Conclusions: L. iners dominance of the vaginal microbiota at 16 weeks of gestation is a risk factor for preterm birth, whereas L. crispatus dominance is protective against preterm birth. Vaginal progesterone does not appear to impact the pregnancy vaginal microbiota. Patients and clinicians who may be concerned about "infection risk" associated with the use of a vaginal pessary during high-risk pregnancy can be reassured.
Keywords: Cervical length; Lactobacillus; Preterm birth; Progesterone; Vaginal microbiome.
Figures
References
-
- Causes of child mortality [http://www.who.int/gho/child_health/mortality/causes/en/]. Accessed 7 July 2016.
-
- Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, Cousens S, Mathers C, Black RE. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385(9966):430–440. doi: 10.1016/S0140-6736(14)61698-6. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
