

AF Ablation Guided by Spatiotemporal Electrogram Dispersion Without Pulmonary Vein Isolation: A Wholly Patient-Tailored Approach
- PMID: 28104073
- PMCID: PMC5568427
- DOI: 10.1016/j.jacc.2016.10.065
AF Ablation Guided by Spatiotemporal Electrogram Dispersion Without Pulmonary Vein Isolation: A Wholly Patient-Tailored Approach
Abstract
Background: The use of intracardiac electrograms to guide atrial fibrillation (AF) ablation has yielded conflicting results.
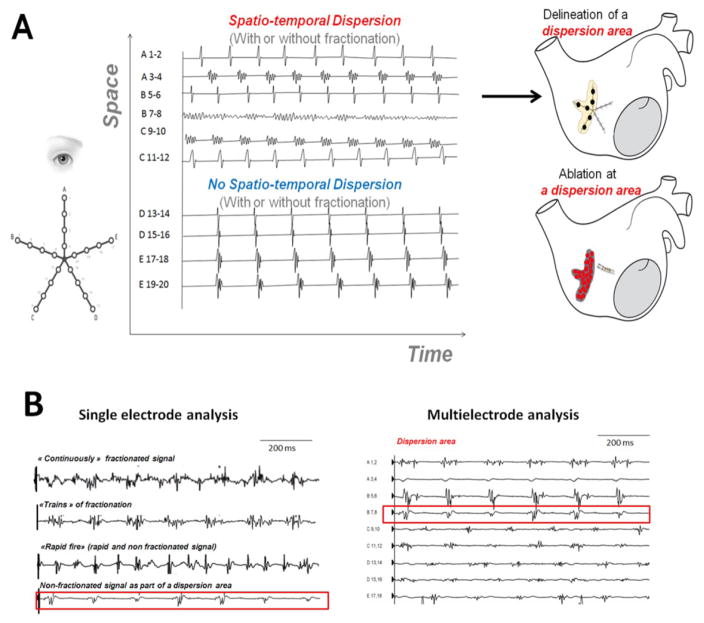
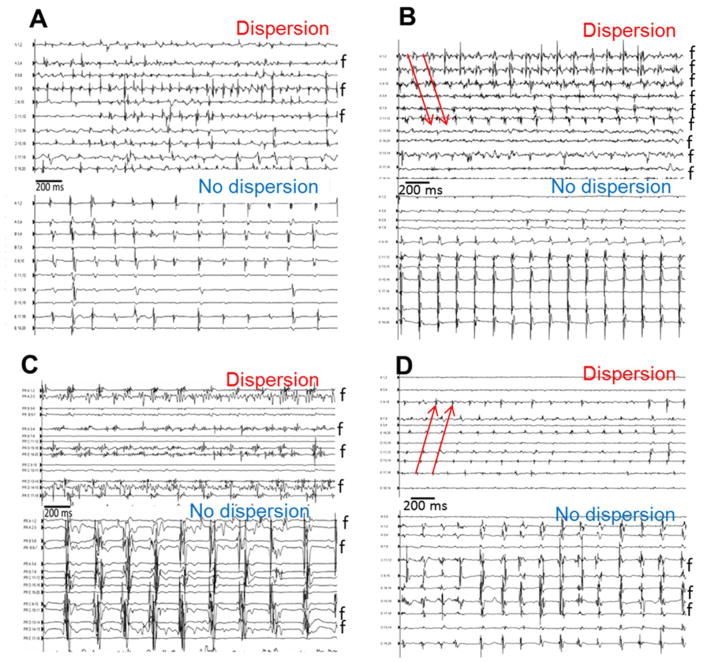
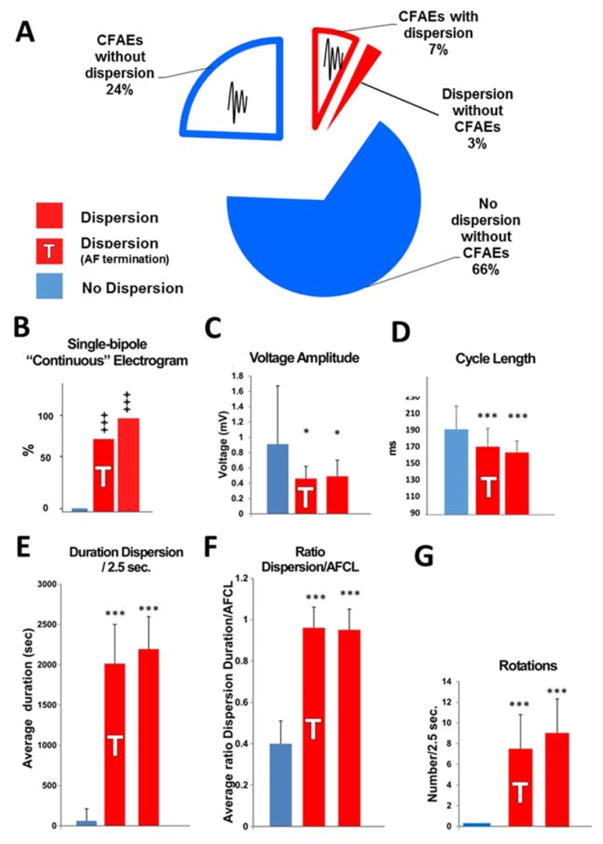
Objectives: The authors evaluated the usefulness of spatiotemporal dispersion, a visually recognizable electric footprint of AF drivers, for the ablation of all forms of AF.
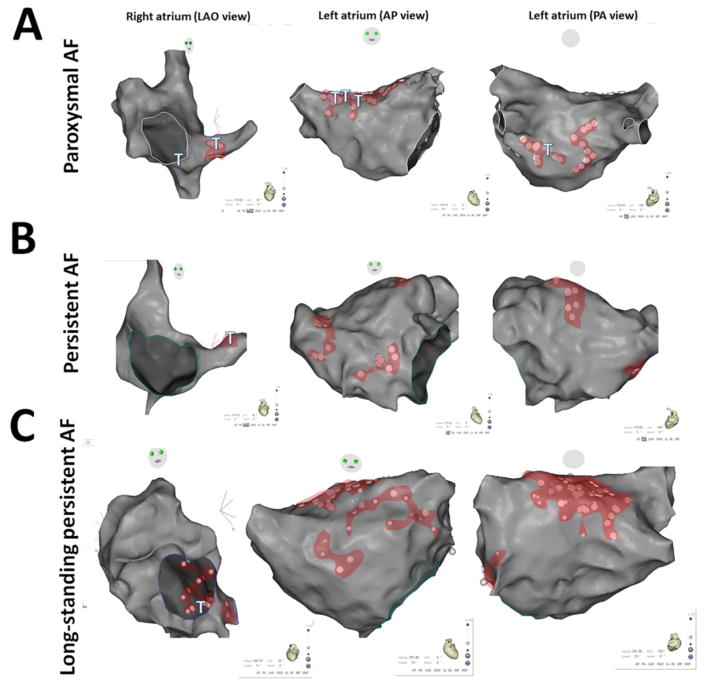
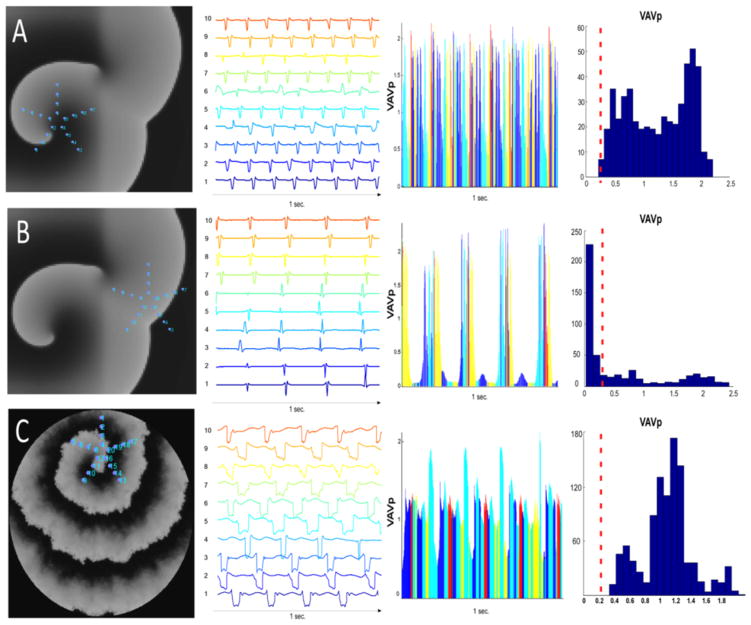
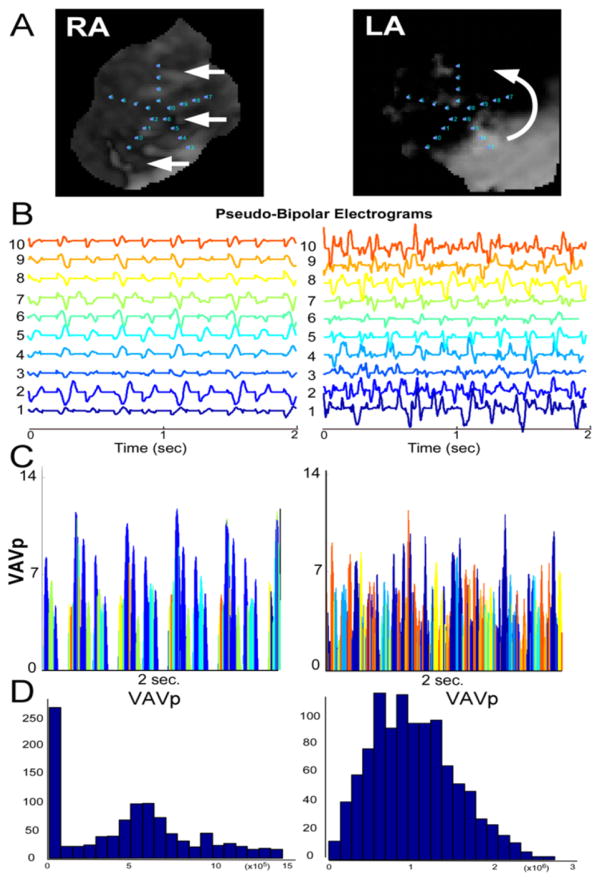
Methods: The authors prospectively enrolled 105 patients admitted for AF ablation. AF was sequentially mapped in both atria with a 20-pole PentaRay catheter. The authors tagged and ablated only regions displaying electrogram dispersion during AF. Results were compared to a validation set in which a conventional ablation approach was used (pulmonary vein isolation/stepwise approach). To establish the mechanism underlying spatiotemporal dispersion of AF electrograms, the authors conducted realistic numerical simulations of AF drivers in a 2-dimensional model and optical mapping of ovine atrial scar-related AF.
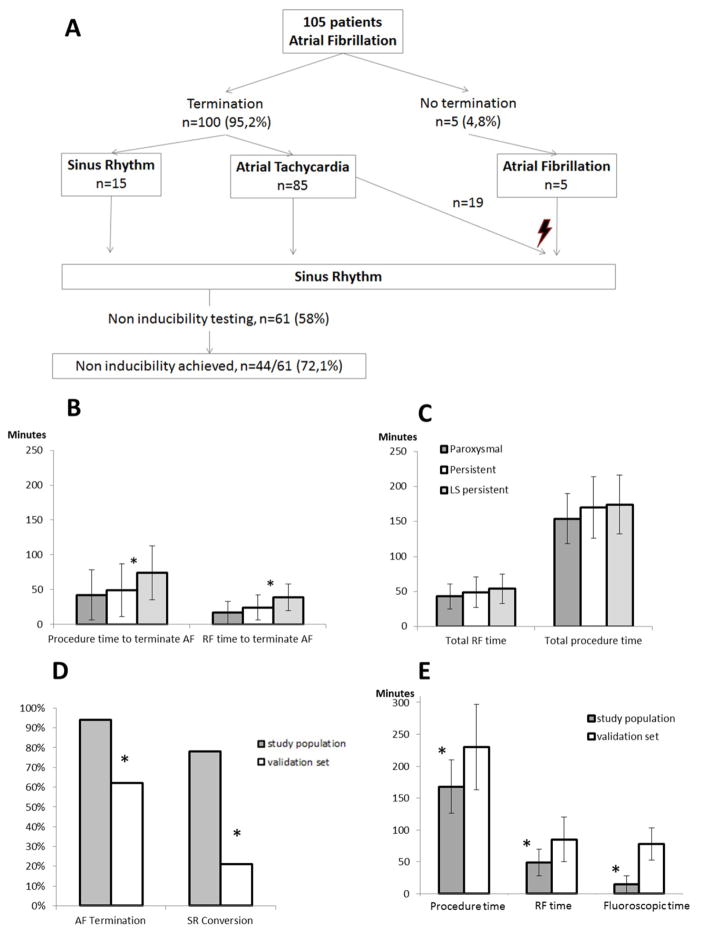
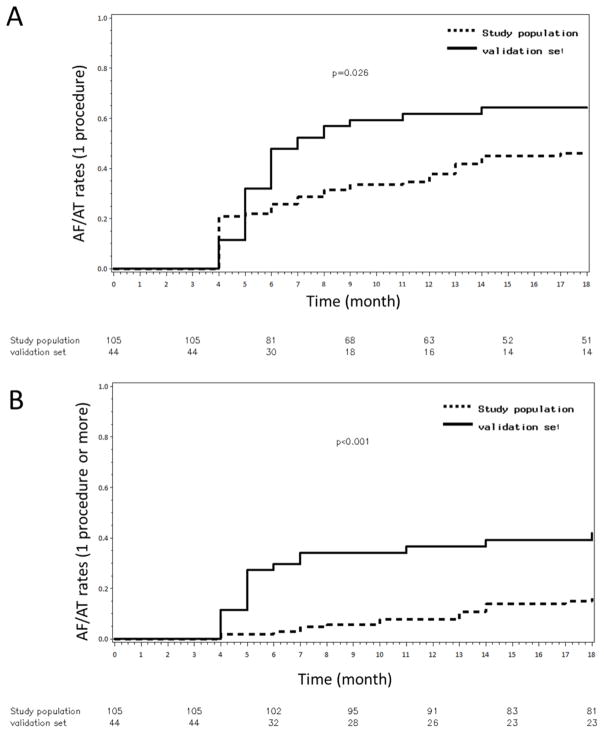
Results: Ablation at dispersion areas terminated AF in 95% of the 105 patients. After ablation of 17 ± 10% of the left atrial surface and 18 months of follow-up, the atrial arrhythmia recurrence rate was 15% after 1.4 ± 0.5 procedures per patient versus 41% in the validation set after 1.5 ± 0.5 procedures per patient (arrhythmia free-survival: 85% vs. 59%; log-rank p < 0.001). Compared with the validation set, radiofrequency times (49 ± 21 min vs. 85 ± 34.5 min; p = 0.001) and procedure times (168 ± 42 min vs. 230 ± 67 min; p < 0.0001) were shorter. In simulations and optical mapping experiments, virtual PentaRay recordings demonstrated that electrogram dispersion is mostly recorded in the vicinity of a driver.
Conclusions: The clustering of intracardiac electrograms exhibiting spatiotemporal dispersion is indicative of AF drivers. Their ablation allows for a nonextensive and patient-tailored approach to AF ablation. (Substrate Ablation Guided by High Density Mapping in Atrial Fibrillation [SUBSTRATE HD]; NCT02093949).
Keywords: cycle length; dispersion driver; fractionated; mapping; sinus rhythm.
Copyright © 2017 American College of Cardiology Foundation. All rights reserved.
Figures
Comment in
-
Substrate Ablation Without Pulmonary Vein Isolation: A Reasonable Proposition for Atrial Fibrillation Ablation?J Am Coll Cardiol. 2017 Jan 24;69(3):322-324. doi: 10.1016/j.jacc.2016.11.022. J Am Coll Cardiol. 2017. PMID: 28104074 No abstract available.
-
History Repeating?: The Logics of History.J Am Coll Cardiol. 2017 Jun 27;69(25):3121-3122. doi: 10.1016/j.jacc.2017.02.077. J Am Coll Cardiol. 2017. PMID: 28641803 No abstract available.
-
Reply: History Repeating? The Logics of History.J Am Coll Cardiol. 2017 Jun 27;69(25):3122-3123. doi: 10.1016/j.jacc.2017.03.607. J Am Coll Cardiol. 2017. PMID: 28641804 No abstract available.
References
-
- Verma A, Jiang C, Betts TR, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372:1812–1822. - PubMed
-
- Wong KCK, Paisey JR, Sopher M, et al. No Benefit OF Complex Fractionated Atrial Electrogram (CFAE) Ablation in Addition to Circumferential Pulmonary Vein Ablation and Linear Ablation: BOCA Study. Circ Arrhythm Electrophysiol. 2015 CIRCEP.114.002504. - PubMed
-
- Oral H, Chugh A, Good E, et al. Radiofrequency catheter ablation of chronic atrial fibrillation guided by complex electrograms. Circulation. 2007;115:2606–2612. - PubMed
-
- Providência R, Lambiase PD, Srinivasan N, et al. Is There Still a Role for Complex Fractionated Atrial Electrogram Ablation in Addition to Pulmonary Vein Isolation in Patients With Paroxysmal and Persistent Atrial Fibrillation?: Meta-Analysis of 1415 Patients. Circ Arrhythm Electrophysiol. 2015;8:1017–1029. - PubMed
-
- Vogler J, Willems S, Sultan A, et al. Pulmonary Vein Isolation Versus Defragmentation: The CHASE-AF Clinical Trial. J Am Coll Cardiol. 2015;66:2743–2752. - PubMed
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
