

Next Generation Flow for highly sensitive and standardized detection of minimal residual disease in multiple myeloma
- PMID: 28104919
- PMCID: PMC5629369
- DOI: 10.1038/leu.2017.29
Next Generation Flow for highly sensitive and standardized detection of minimal residual disease in multiple myeloma
Abstract
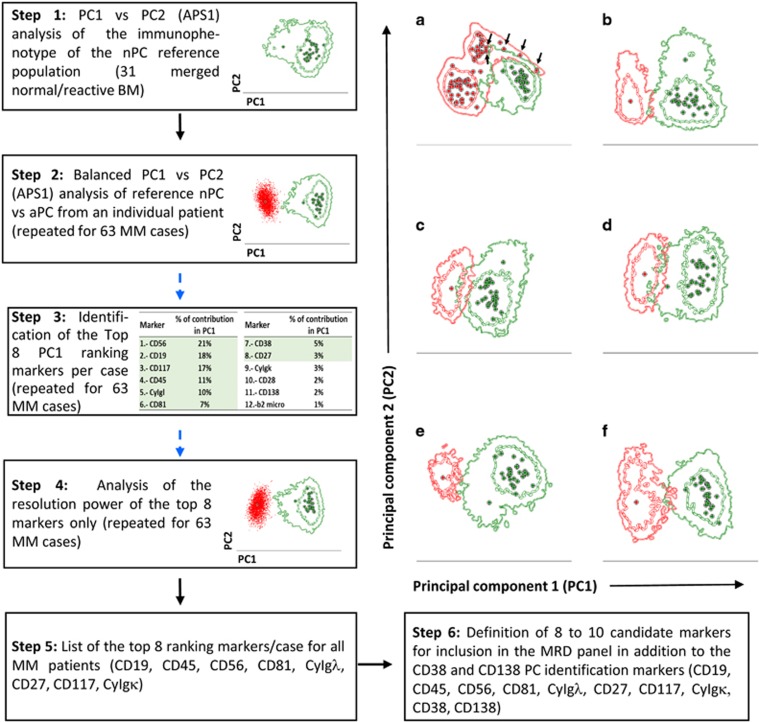
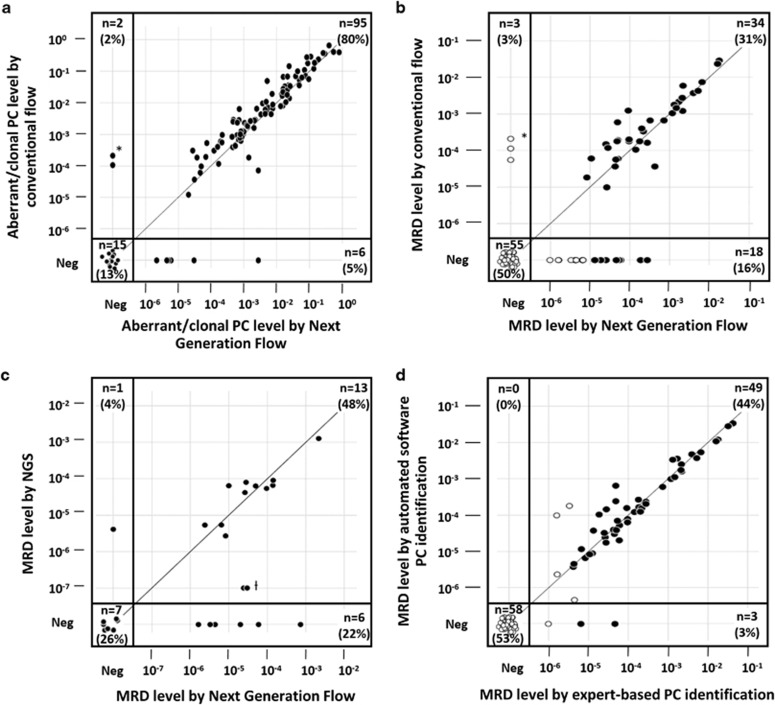
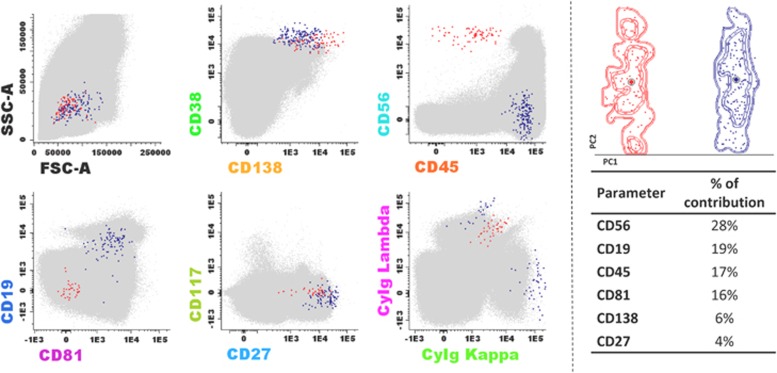
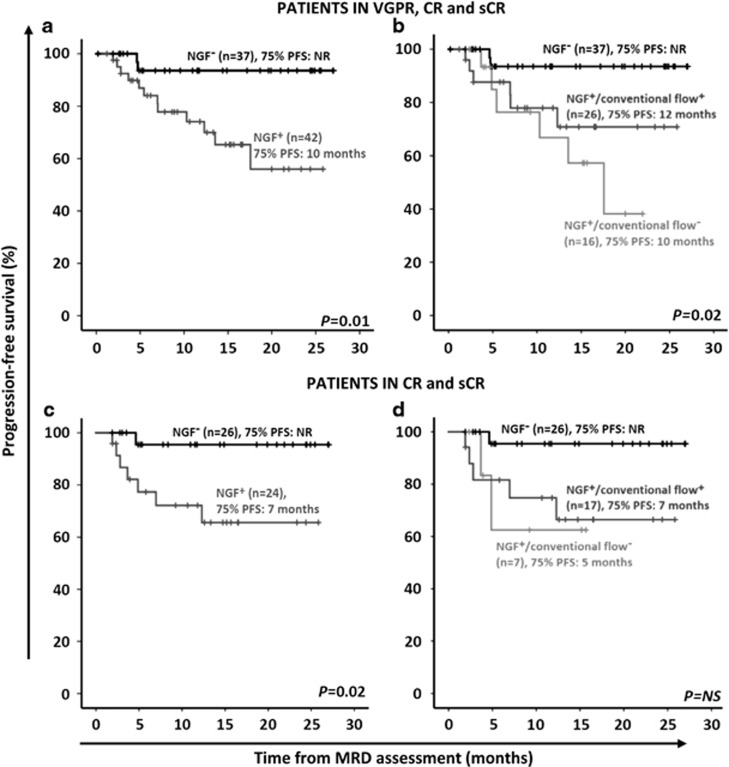
Flow cytometry has become a highly valuable method to monitor minimal residual disease (MRD) and evaluate the depth of complete response (CR) in bone marrow (BM) of multiple myeloma (MM) after therapy. However, current flow-MRD has lower sensitivity than molecular methods and lacks standardization. Here we report on a novel next generation flow (NGF) approach for highly sensitive and standardized MRD detection in MM. An optimized 2-tube 8-color antibody panel was constructed in five cycles of design-evaluation-redesign. In addition, a bulk-lysis procedure was established for acquisition of ⩾107 cells/sample, and novel software tools were constructed for automatic plasma cell gating. Multicenter evaluation of 110 follow-up BM from MM patients in very good partial response (VGPR) or CR showed a higher sensitivity for NGF-MRD vs conventional 8-color flow-MRD -MRD-positive rate of 47 vs 34% (P=0.003)-. Thus, 25% of patients classified as MRD-negative by conventional 8-color flow were MRD-positive by NGF, translating into a significantly longer progression-free survival for MRD-negative vs MRD-positive CR patients by NGF (75% progression-free survival not reached vs 7 months; P=0.02). This study establishes EuroFlow-based NGF as a highly sensitive, fully standardized approach for MRD detection in MM which overcomes the major limitations of conventional flow-MRD methods and is ready for implementation in routine diagnostics.
Conflict of interest statement
G-EG and RF are employees of Cytognos SL, Salamanca, Spain. JJMvD received research support and traveling support from Roche, Amgen and Becton Dickinson. SB received research support from Roche, Celgene, Becton Dickinson and AbbVie as well as honoraria from Roche and AbbVie. JF-M, LS-F, OG-S, J-JP-M, AC-M, CJ, JM-L, M-VM, VvdV, JC, LS, NP, M-BV, RGS, MG, RP, M-CdC, JB, J-JL, CA, AB, AG-M, JL, PL, CA-S, JS-M, BD and AO declare no conflict of interest.
Figures
References
-
- Lahuerta JJ, Mateos MV, Martinez-Lopez J, Rosinol L, Sureda A, de la Rubia J et al. Influence of pre- and post-transplantation responses on outcome of patients with multiple myeloma: sequential improvement of response and achievement of complete response are associated with longer survival. J Clin Oncol 2008; 26: 5775–5782. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
