

Bone Density in the Obese Child: Clinical Considerations and Diagnostic Challenges
- PMID: 28105511
- PMCID: PMC5395312
- DOI: 10.1007/s00223-016-0233-4
Bone Density in the Obese Child: Clinical Considerations and Diagnostic Challenges
Abstract
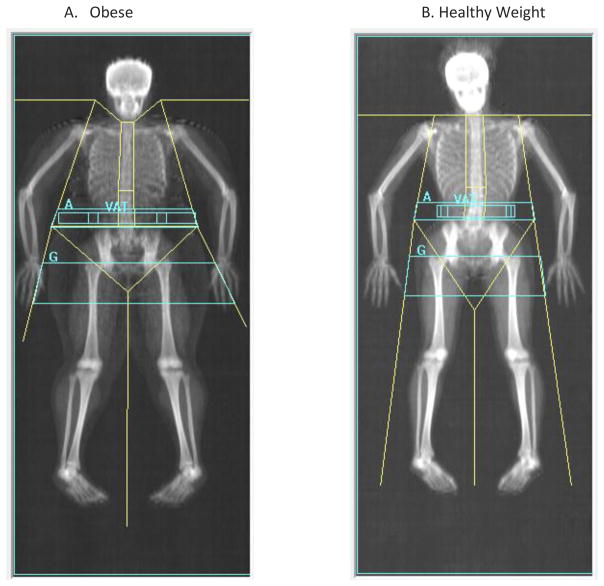
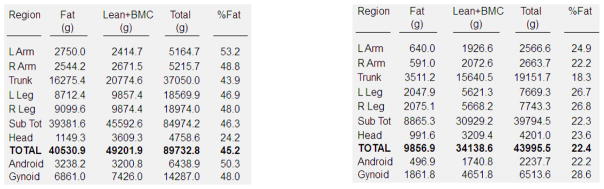
The prevalence of obesity in children has reached epidemic proportions. Concern about bone health in obese children, in part, derives from the potentially increased fracture risk associated with obesity. Additional risk factors that affect bone mineral accretion, may also contribute to obesity, such as low physical activity and nutritional factors. Consequences of obesity, such as inflammation, insulin resistance, and non-alcoholic fatty liver disease, may also affect bone mineral acquisition, especially during the adolescent years when rapid increases in bone contribute to attaining peak bone mass. Further, numerous pediatric health conditions are associated with excess adiposity, altered body composition, or endocrine disturbances that can affect bone accretion. Thus, there is a multitude of reasons for considering clinical assessment of bone health in an obese child. Multiple diagnostic challenges affect the measurement of bone density and its interpretation. These include greater precision error, difficulty in positioning, and the effects of increased lean and fat tissue on bone health outcomes. Future research is required to address these issues to improve bone health assessment in obese children.
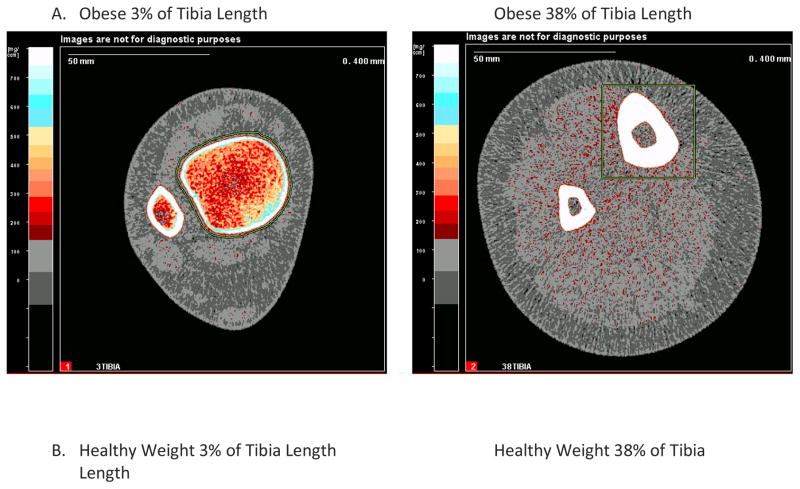
Keywords: Body composition; Children; Dual-energy X-ray absorptiometry; Fracture; Obesity; Peripheral quantitative computed tomography.
Conflict of interest statement
Jennifer Kelley has nothing to disclose.
Nicola Crabtree has nothing to disclose.
Babette Zemel has nothing to disclose.
Figures
Similar articles
-
Non-alcoholic fatty liver disease is associated with low bone mineral density in obese children.Aliment Pharmacol Ther. 2012 Jan;35(2):248-54. doi: 10.1111/j.1365-2036.2011.04924.x. Epub 2011 Nov 24. Aliment Pharmacol Ther. 2012. PMID: 22111971 Free PMC article.
-
Bone mineral density and body composition in boys with distal forearm fractures: a dual-energy x-ray absorptiometry study.J Pediatr. 2001 Oct;139(4):509-15. doi: 10.1067/mpd.2001.116297. J Pediatr. 2001. PMID: 11598596
-
Measurement error of DXA: interpretation of fat and lean mass changes in obese and non-obese children.J Clin Densitom. 2006 Jul-Sep;9(3):335-40. doi: 10.1016/j.jocd.2006.03.016. Epub 2006 May 15. J Clin Densitom. 2006. PMID: 16931353
-
The Bones of Children With Obesity.Front Endocrinol (Lausanne). 2020 Apr 24;11:200. doi: 10.3389/fendo.2020.00200. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32390939 Free PMC article. Review.
-
Dual-energy X-ray absorptiometry body composition in patients with secondary osteoporosis.Eur J Radiol. 2016 Aug;85(8):1493-8. doi: 10.1016/j.ejrad.2016.03.018. Epub 2016 Mar 22. Eur J Radiol. 2016. PMID: 27048946 Review.
Cited by
-
The Role of Obesity in Pediatric Orthopedics.J Am Acad Orthop Surg Glob Res Rev. 2019 May 8;3(5):e036. doi: 10.5435/JAAOSGlobal-D-19-00036. eCollection 2019 May. J Am Acad Orthop Surg Glob Res Rev. 2019. PMID: 31321371 Free PMC article.
-
Relationship of cardiometabolic risk biomarkers with DXA and pQCT bone health outcomes in young girls.Bone. 2019 Mar;120:452-458. doi: 10.1016/j.bone.2018.12.013. Epub 2018 Dec 18. Bone. 2019. PMID: 30572143 Free PMC article.
-
Relative contributions of lean and fat mass to bone strength in young Hispanic and non-Hispanic girls.Bone. 2018 Aug;113:144-150. doi: 10.1016/j.bone.2018.05.023. Epub 2018 May 22. Bone. 2018. PMID: 29800691 Free PMC article.
-
Muscular Fitness Mediates the Association between 25-Hydroxyvitamin D and Areal Bone Mineral Density in Children with Overweight/Obesity.Nutrients. 2019 Nov 14;11(11):2760. doi: 10.3390/nu11112760. Nutrients. 2019. PMID: 31739435 Free PMC article.
-
The "Burden" of Childhood Obesity on Bone Health: A Look at Prevention and Treatment.Nutrients. 2025 Jan 29;17(3):491. doi: 10.3390/nu17030491. Nutrients. 2025. PMID: 39940349 Free PMC article. Review.
References
-
- Ogden CL, Carroll MD, Fryar CD, Flegal KM. Prevalence of Obesity Among Adults and Youth: United States, 2011–2014. NCHS Data Brief. 2015:1–8. - PubMed
-
- de Onis M, Blossner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr. 2010;92:1257–1264. - PubMed
-
- Deckelbaum RJ, Williams CL. Childhood obesity: the health issue. Obes Res. 2001;9(Suppl 4):239S–243S. - PubMed
-
- Baxter-Jones AD, Faulkner RA, Forwood MR, Mirwald RL, Bailey DA. Bone mineral accrual from 8 to 30 years of age: an estimation of peak bone mass. J Bone Miner Res. 2011;26:1729–1739. - PubMed
-
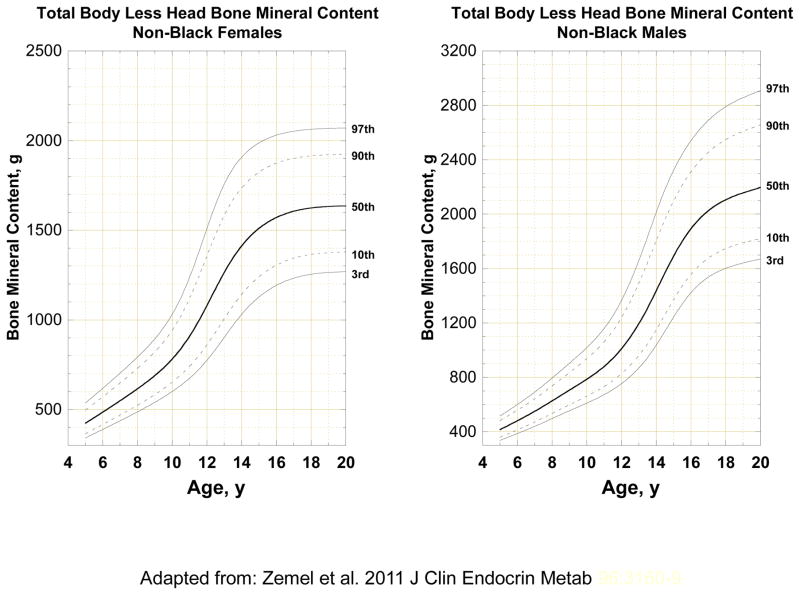
- Gordon CM, Bachrach LK, Carpenter TO, Crabtree N, El-Hajj Fuleihan G, Kutilek S, Lorenc RS, Tosi LL, Ward KA, Ward LM, Kalkwarf HJ. Dual energy X-ray absorptiometry interpretation and reporting in children and adolescents: the 2007 ISCD Pediatric Official Positions. J Clin Densitom. 2008;11:43–58. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
