

Radio-pathological correlation of organizing pneumonia (OP): a pictorial review
- PMID: 28106480
- PMCID: PMC5601538
- DOI: 10.1259/bjr.20160723
Radio-pathological correlation of organizing pneumonia (OP): a pictorial review
Abstract
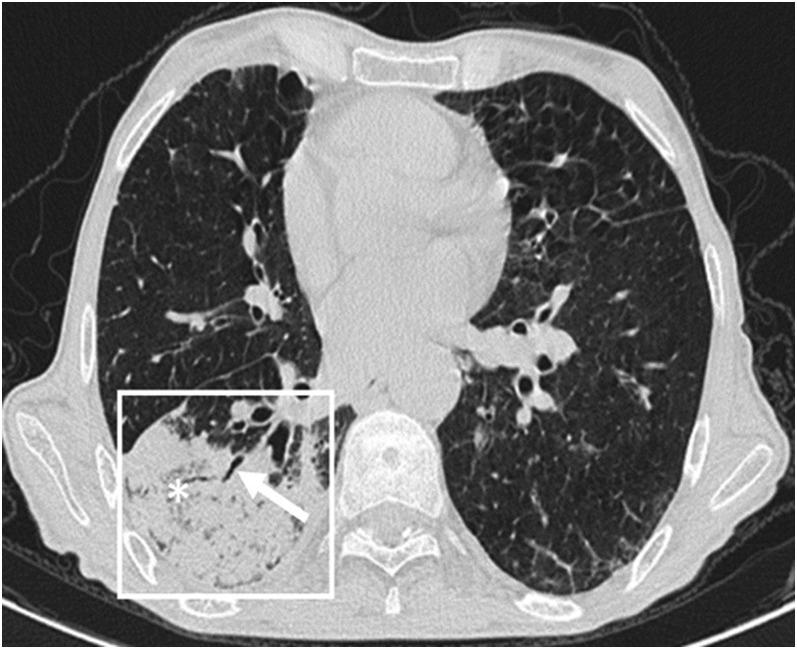
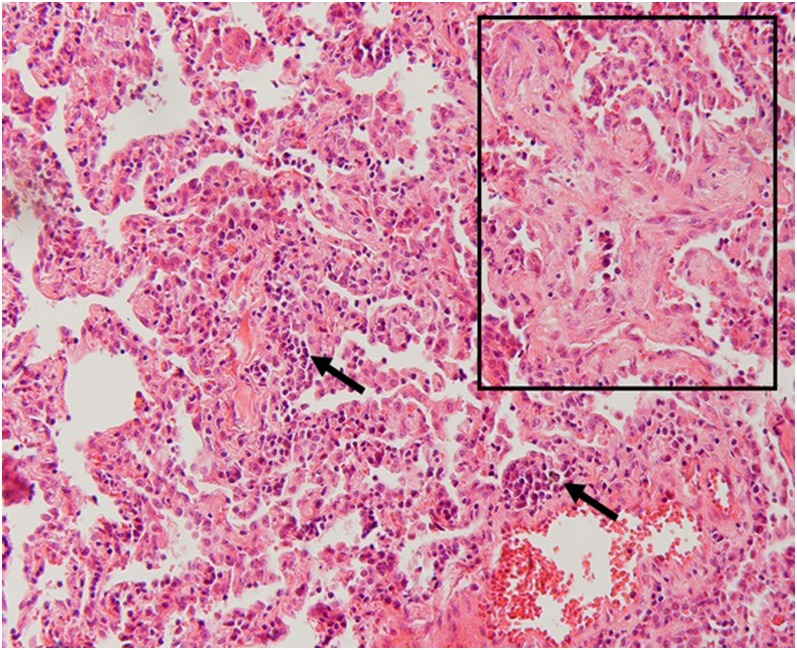
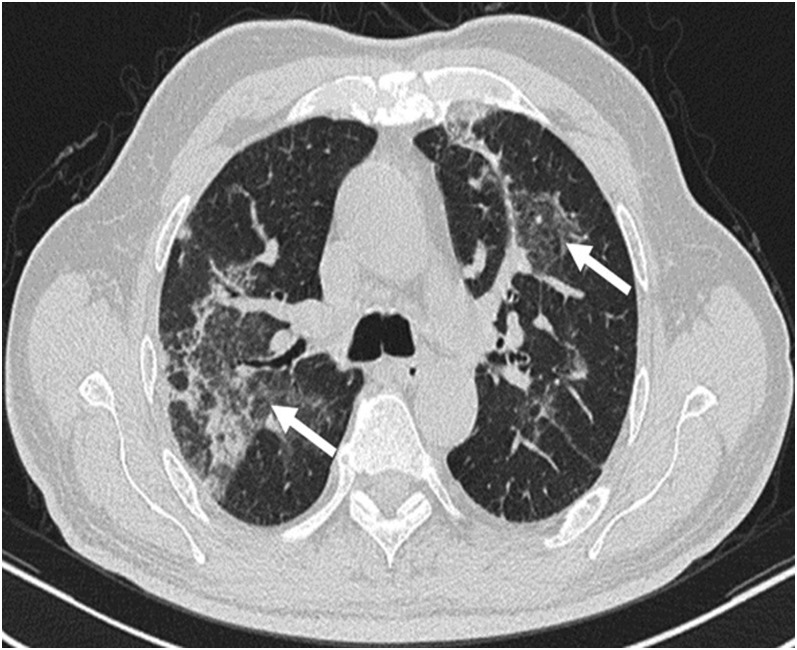
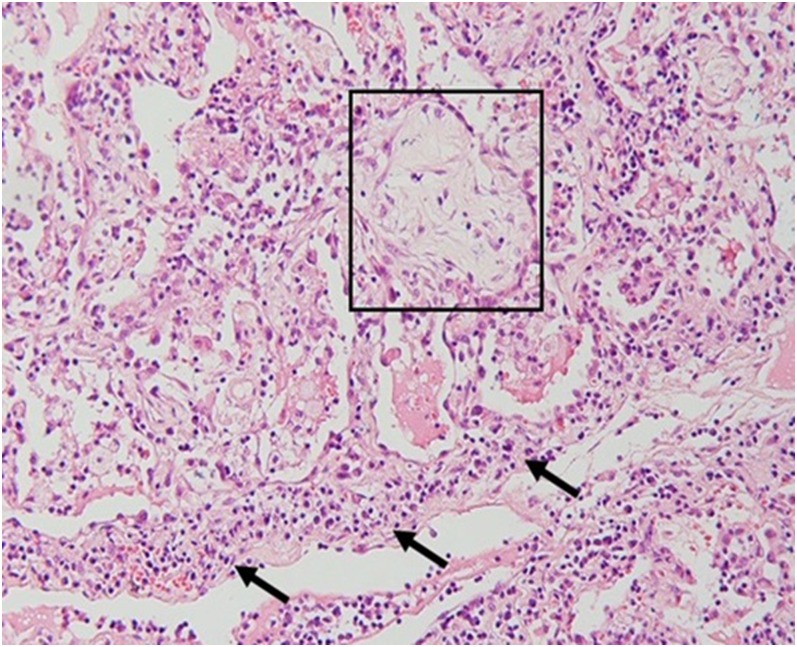
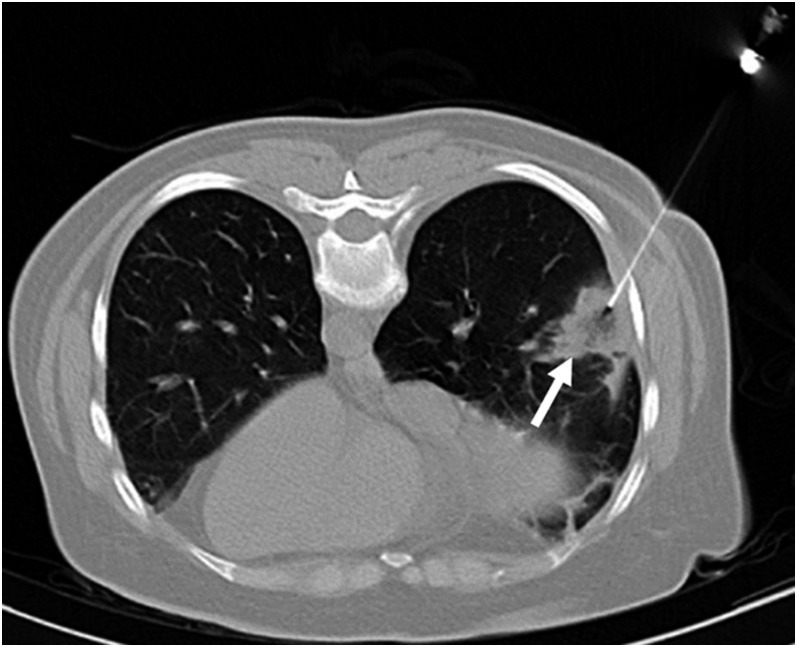
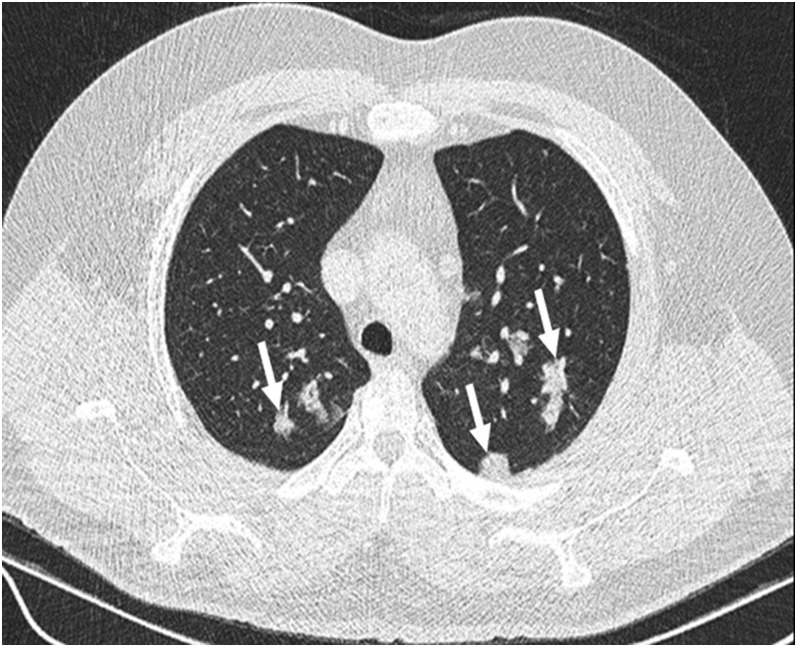
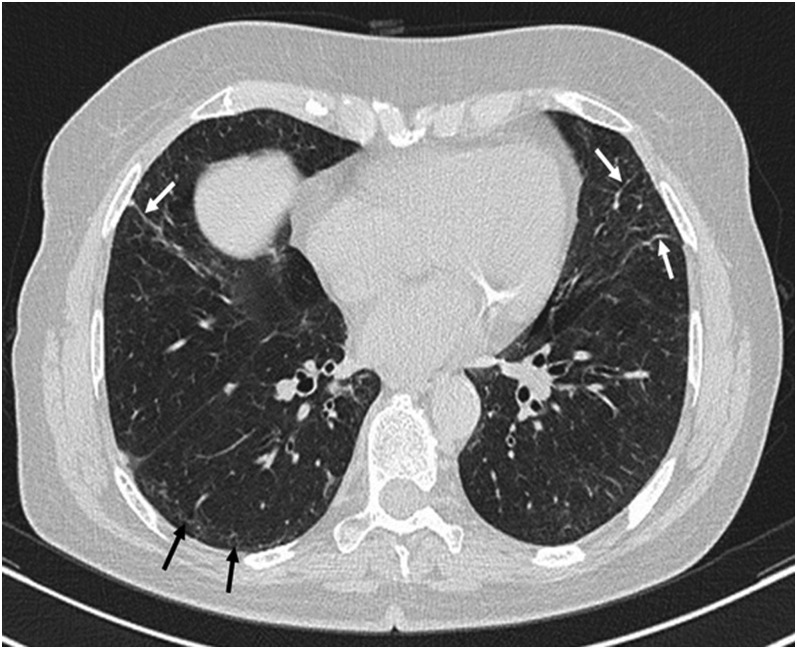
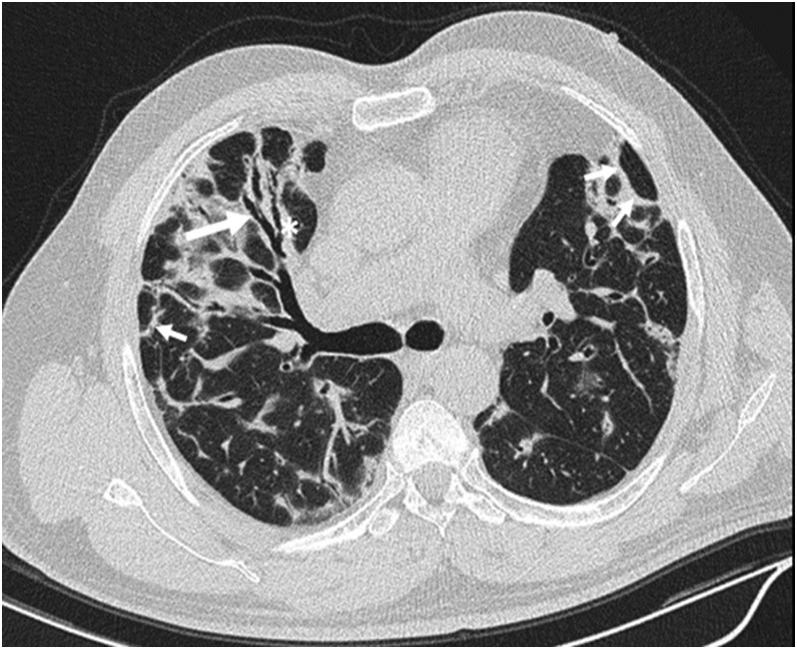
Since the description of cryptogenic organizing pneumonia in 1983 by Davison et al and the subsequent report on bronchiolitis obliterans organizing pneumonia by Epler et al, some reports have been published regarding the imaging features of organizing pneumonia (OP). In this pictorial review, we aimed to describe and illustrate different manifestations of OP on high-resolution CT (HRCT) accompanied by their histopathological correlations for a better comprehension of pathomechanism of the radiological findings. The main HRCT findings in OP include: consolidation, ground-glass opacification, perilobular opacity, reversed halo opacity, nodule or mass, parenchymal bands, bronchial wall thickening, bronchial dilatation, mediastinal lymphadenopathy and pleural effusion. In addition, we discuss the radiological differential diagnosis for each manifestation, as well as imaging evolution during patient follow-up, and two OP-related entities: the possibility of non-specific interstitial pneumonia development following OP and a relatively new rare entity related to OP called acute fibrinous and organizing pneumonia. For radiologists and physicians, a detailed knowledge of the potential radiological manifestations in OP is crucial for making a correct diagnosis and managing the patient properly. Moreover, some unnecessary lung biopsies will be avoided.
Figures

References
-
- Travis WD, Costabel U, Hansell DM, King TE, Jr, Lynch DA, Nicholson AG, et al. ; ATS/ERS Committee on Idiopathic Interstitial Pneumonias. An official American Thoracic Society/European Respiratory Society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med 2013; 188: 733–48. doi: https://doi.org/10.1164/rccm.201308-1483ST - DOI - PMC - PubMed
-
- Mueller-Mang C, Grosse C, Schmid K, Stiebellehner L, Bankier AA. What every radiologist should know about idiopathic interstitial pneumonias. RadioGraphics 2007; 27: 595–615. - PubMed
-
- Kim SJ, Lee KS, Ryu YH, Yoon YC, Choe KO, Kim TS, et al. Reversed halo sign on high-resolution CT of cryptogenic organizing pneumonia: diagnostic implications. AJR Am J Roentgenol 2003; 180: 1251–4. doi: https://doi.org/10.2214/ajr.180.5.1801251 - DOI - PubMed
-
- Müller NL, Staples CA, Miller RR. Bronchiolitis obliterans organizing pneumonia: CT features in 14 patients. AJR Am J Roentgenol 1990; 154: 983–7. - PubMed
-
- Lee KS, Kullnig P, Hartman TE, Müller NL. Cryptogenic organizing pneumonia: CT findings in 43 patients. AJR Am J Roentgenol 1994; 162: 543–6. doi: https://doi.org/10.2214/ajr.162.3.8109493 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
