

Management strategies for atrial fibrillation
- PMID: 28106485
- PMCID: PMC5298423
- DOI: 10.1177/0141076816677857
Management strategies for atrial fibrillation
Abstract
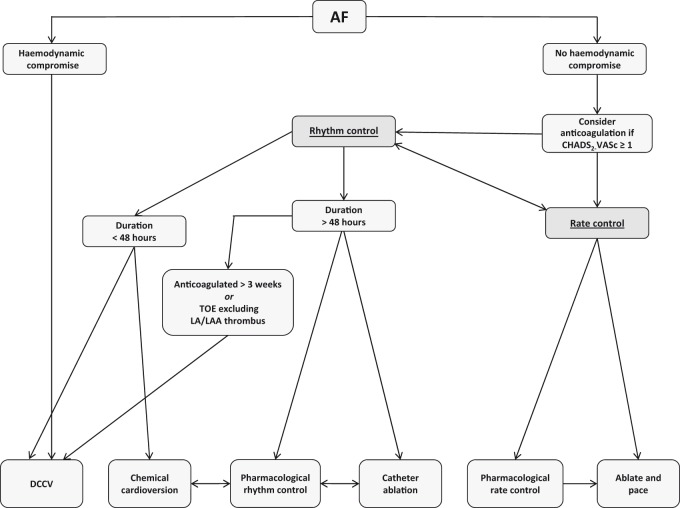
Atrial fibrillation is the most prevalent cardiac arrhythmia, affecting 10% of those aged over 80 years. Despite multiple treatment options, it remains an independent prognostic marker of mortality due to its association with clinical sequelae, particularly cerebrovascular events. Management can be broadly divided into treatment of the arrhythmia, via rhythm or rate control, and stroke thromboprophylaxis via anticoagulation. Traditional options for pharmacotherapy include negatively chronotropic drugs such as β-blockers, and/or arrhythmia-modifying drugs such as amiodarone. More recently, catheter ablation has emerged as a suitable alternative for selected patients. Additionally, there has been extensive research to assess the role of novel oral anticoagulants as alternatives to warfarin therapy. There is mounting evidence to suggest that they provide comparable efficacy, while being associated with lower bleeding complications. While these findings are promising, recent controversies have arisen with the use of novel oral anticoagulants. Further research is warranted to fully elucidate mechanisms and establish antidotes so that treatment options can be appropriately directed.
Keywords: Atrial fibrillation; arrhythmia-modifying drugs; catheter ablation; novel anticoagulants; warfarin.
Figures
References
-
- Naccarelli GV, Varker H, Lin J, Schulman KL. Increasing prevalence of atrial fibrillation and flutter in the United States. Am J Cardiol 2009; 104: 1534–1539. - PubMed
-
- European Heart Rhythm Association Guidelines for the management of atrial fibrillation: the task force for the management of atrial fibrillation of the European Society of Cardiology (ESC). Eur Heart 2010; 31: 2369–2429. - PubMed
-
- Nault I, Miyazaki S, Forclaz A, Wright M, Jadidi A, Jais P, et al. Drugs versus ablation for the treatment of atrial fibrillation: the evidence supporting catheter ablation. Eur Heart J 2010; 31: 1046–1054. - PubMed
-
- Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998; 339: 659–666. - PubMed
-
- Verma A, Jiang CY, Betts TR, Chen J, Deisenhofer I, Mantovan R, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med 2015; 372: 1812–1822. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
