

Planned early delivery versus expectant management for hypertensive disorders from 34 weeks gestation to term
- PMID: 28106904
- PMCID: PMC6465052
- DOI: 10.1002/14651858.CD009273.pub2
Planned early delivery versus expectant management for hypertensive disorders from 34 weeks gestation to term
Abstract
Background: Hypertensive disorders in pregnancy are significant contributors to maternal and perinatal morbidity and mortality. These disorders include well-controlled chronic hypertension, gestational hypertension (pregnancy-induced hypertension) and mild pre-eclampsia. The definitive treatment for these disorders is planned early delivery and the alternative is to manage the pregnancy expectantly if severe uncontrolled hypertension is not present, with close maternal and fetal monitoring. There are benefits and risks associated with both, so it is important to establish the safest option.
Objectives: To assess the benefits and risks of a policy of planned early delivery versus a policy of expectant management in pregnant women with hypertensive disorders, at or near term (from 34 weeks onwards).
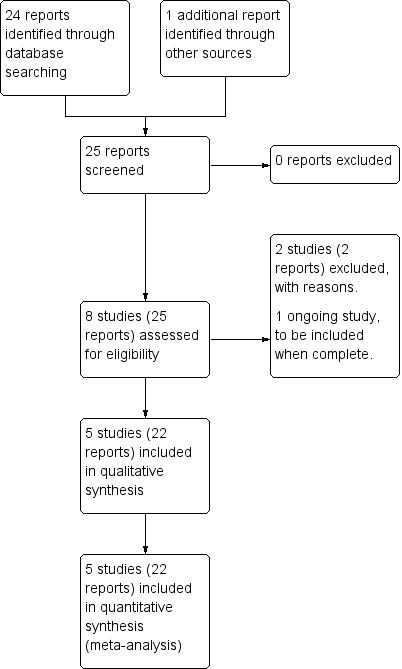
Search methods: We searched Cochrane Pregnancy and Childbirth Trials Register (12 January 2016) and reference lists of retrieved studies.
Selection criteria: Randomised trials of a policy of planned early delivery (by induction of labour or by caesarean section) compared with a policy of delayed delivery ("expectant management") for women with hypertensive disorders from 34 weeks' gestation. Cluster-randomised trials would have been eligible for inclusion in this review, but we found none.Studies using a quasi-randomised design are not eligible for inclusion in this review. Similarly, studies using a cross-over design are not eligible for inclusion, because they are not a suitable study design for investigating hypertensive disorders in pregnancy.
Data collection and analysis: Two review authors independently assessed eligibility and risks of bias. Two review authors independently extracted data. Data were checked for accuracy.
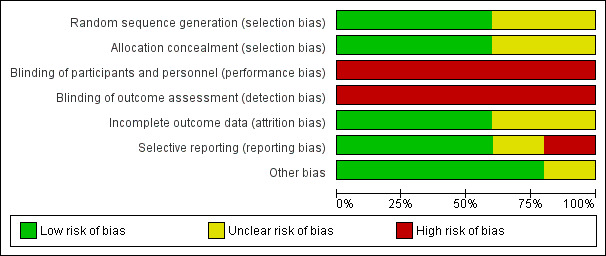
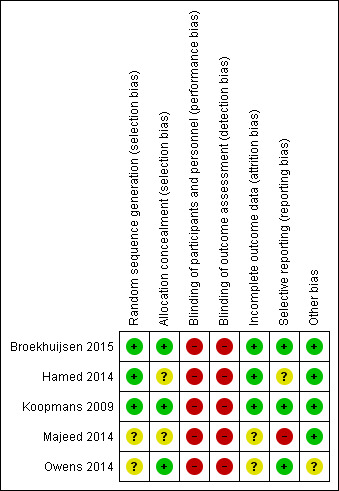
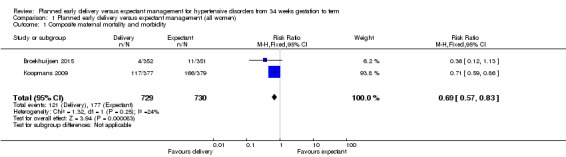
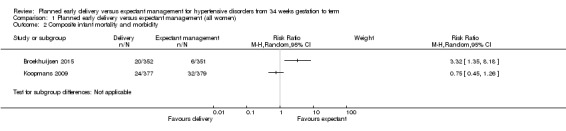
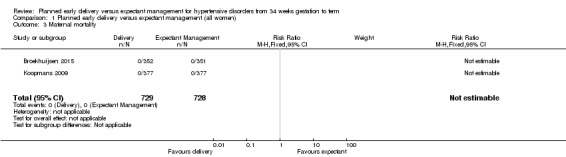
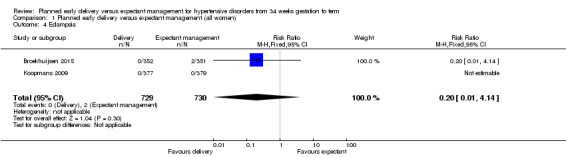
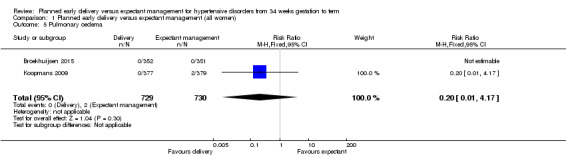
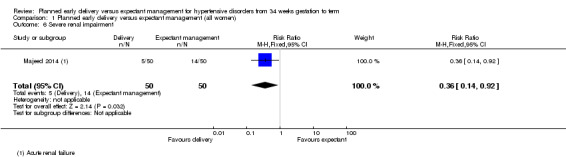
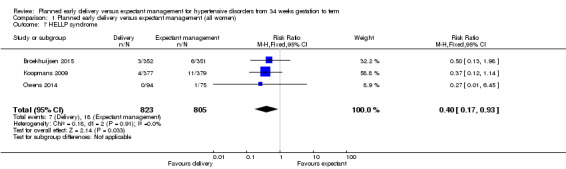
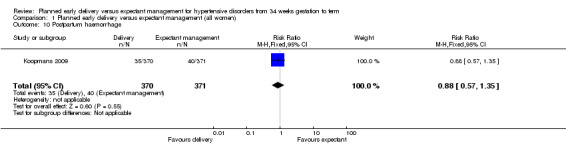
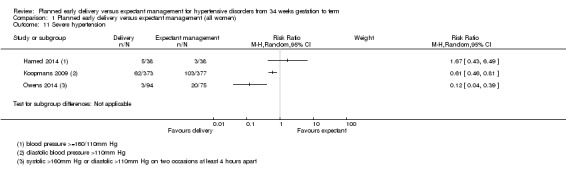
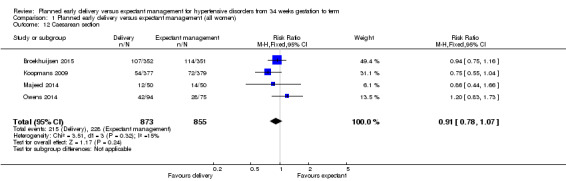
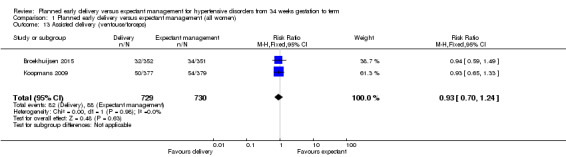
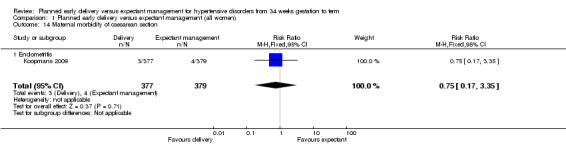
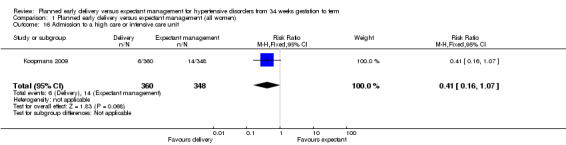
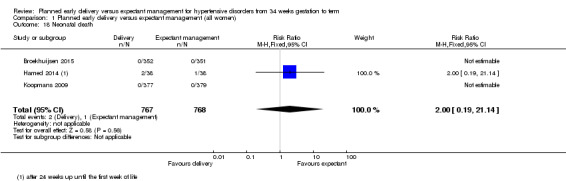
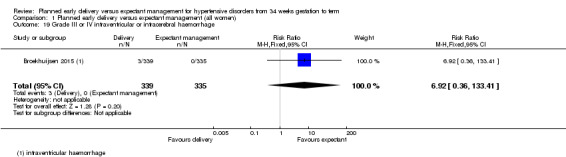
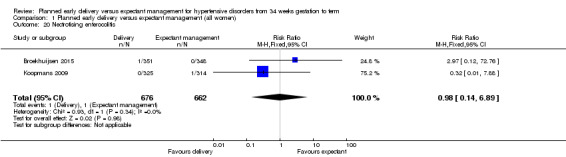
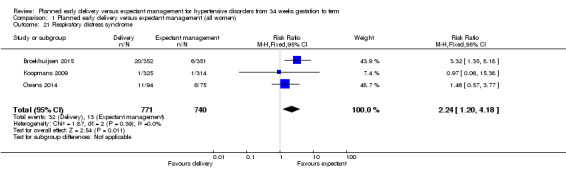
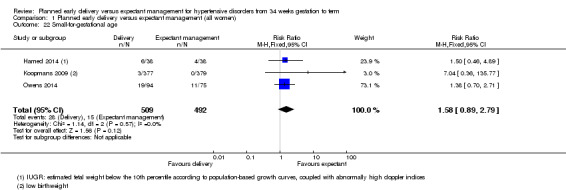
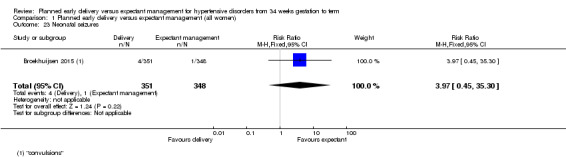
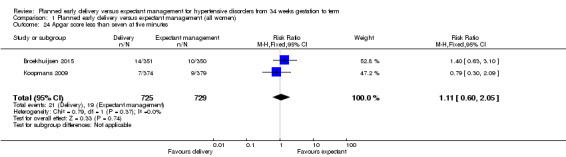
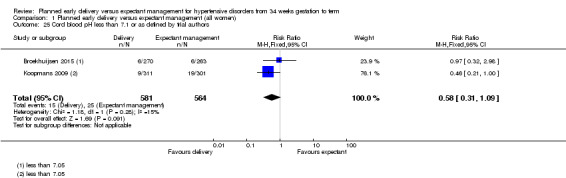
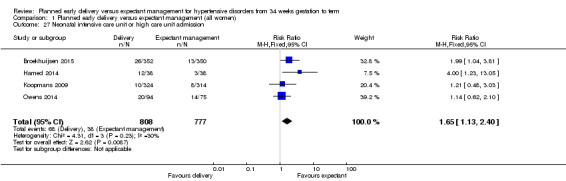
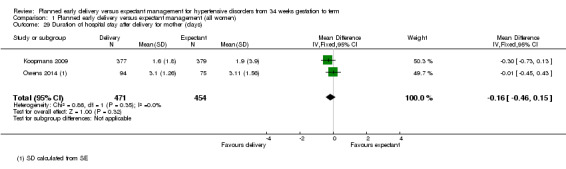
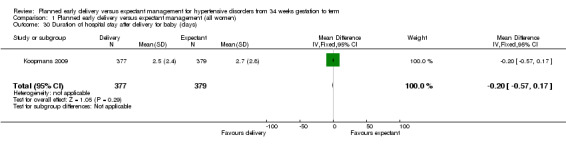
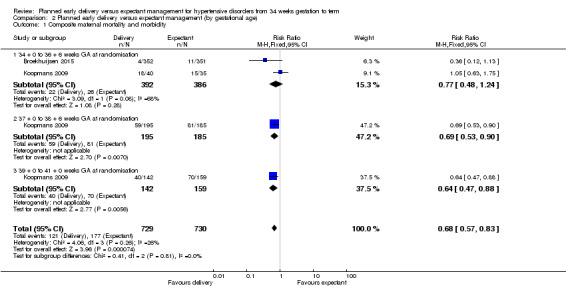
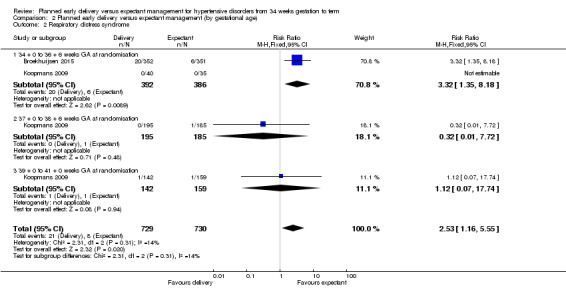
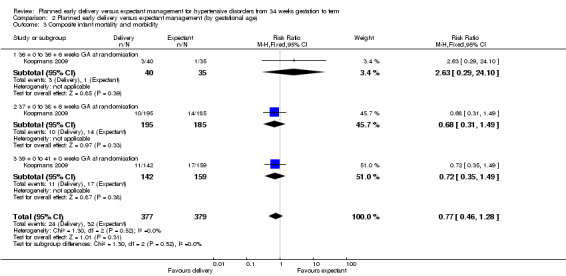
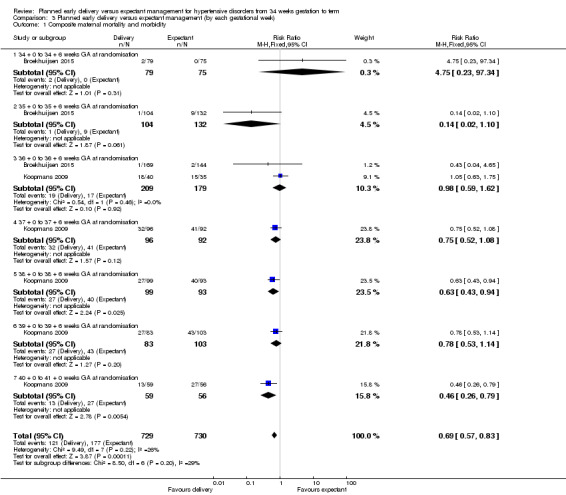
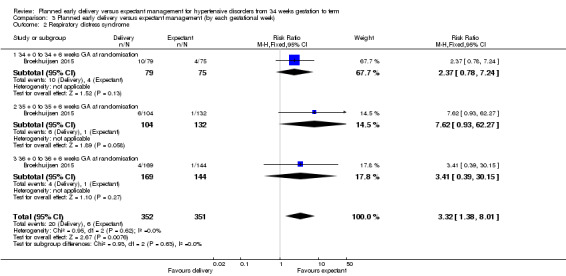
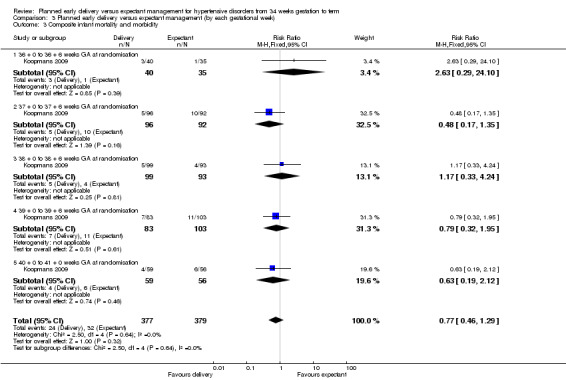
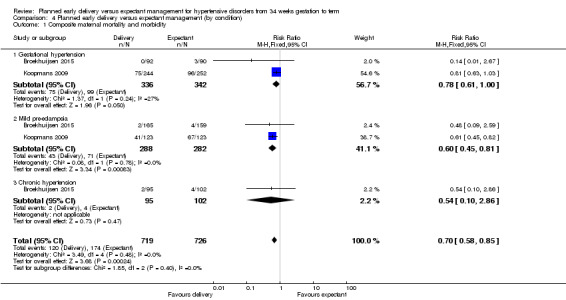
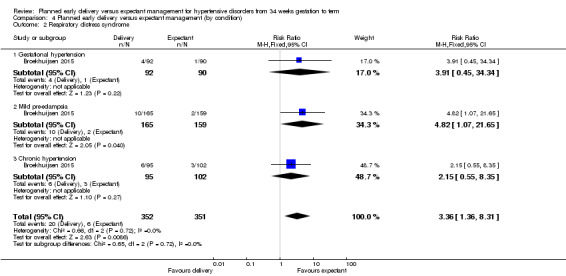
Main results: We included five studies (involving 1819 women) in this review.There was a lower risk of composite maternal mortality and severe morbidity for women randomised to receive planned early delivery (risk ratio (RR) 0.69, 95% confidence interval (CI) 0.57 to 0.83, two studies, 1459 women (evidence graded high)). There were no clear differences between subgroups based on our subgroup analysis by gestational age, gestational week or condition. Planned early delivery was associated with lower risk of HELLP syndrome (RR 0.40, 95% CI 0.17 to 0.93, 1628 women; three studies) and severe renal impairment (RR 0.36, 95% CI 0.14 to 0.92, 100 women, one study).There was not enough information to draw any conclusions about the effects on composite infant mortality and severe morbidity. We observed a high level of heterogeneity between the two studies in this analysis (two studies, 1459 infants, I2 = 87%, Tau2 = 0.98), so we did not pool data in meta-analysis. There were no clear differences between subgroups based on our subgroup analysis by gestational age, gestational week or condition. Planned early delivery was associated with higher levels of respiratory distress syndrome (RR 2.24, 95% CI 1.20 to 4.18, three studies, 1511 infants), and NICU admission (RR 1.65, 95% CI 1.13 to 2.40, four studies, 1585 infants).There was no clear difference between groups for caesarean section (RR 0.91, 95% CI 0.78 to 1.07, 1728 women, four studies, evidence graded moderate), or in the duration of hospital stay for the mother after delivery of the baby (mean difference (MD) -0.16 days, 95% CI -0.46 to 0.15, two studies, 925 women, evidence graded moderate) or for the baby (MD -0.20 days, 95% CI -0.57 to 0.17, one study, 756 infants, evidence graded moderate).Two fairly large, well-designed trials with overall low risk of bias contributed the majority of the evidence. Other studies were at low or unclear risk of bias. No studies attempted to blind participants or clinicians to group allocation, potentially introducing bias as women and staff would have been aware of the intervention and this may have affected aspects of care and decision-making.The level of evidence was graded high (composite maternal mortality and morbidity), moderate (caesarean section, duration of hospital stay after delivery for mother, and duration of hospital stay after delivery for baby) or low (composite infant mortality and morbidity). Where the evidence was downgraded, it was mostly because the confidence intervals were wide, crossing both the line of no effect and appreciable benefit or harm.
Authors' conclusions: For women suffering from hypertensive disorders of pregnancy after 34 weeks, planned early delivery is associated with less composite maternal morbidity and mortality. There is no clear difference in the composite outcome of infant mortality and severe morbidity; however, this is based on limited data (from two trials) assessing all hypertensive disorders as one group.Further studies are needed to look at the different types of hypertensive diseases and the optimal timing of delivery for these conditions. These studies should also include infant and maternal morbidity and mortality outcomes, caesarean section, duration of hospital stay after delivery for mother and duration of hospital stay after delivery for baby.An individual patient meta-analysis on the data currently available would provide further information on the outcomes of the different types of hypertensive disease encountered in pregnancy.
Conflict of interest statement
CK is an author of an included study in this review (Koopmans 2009). All decisions relating to this study (assessment for inclusion/exclusion, risk of bias and data extraction) were carried out by the other members of the review team who are not directly involved in the study.
HW is paid to work on Cochrane reviews by a grant to Cochrane Pregnancy and Childbirth. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
CC: none known.
NN: none known.
Figures
Update of
References
References to studies included in this review
Broekhuijsen 2015 {published data only}
-
- Broekhuijsen K, Langenveld J, Baaren G, Pampus MG, Kaam AH, Groen H, et al. Correction: Induction of labour versus expectant monitoring for gestational hypertension or mild pre‐eclampsia between 34 and 37 weeks’ gestation (HYPITAT‐II): a multicentre, open‐label randomised controlled trial. BMC Pregnancy and Childbirth 2013;13:232. - PMC - PubMed
-
- Broekhuijsen K, Baaren GJ, Pampus M, Ganzevoort W, Sikkema M, Woiski M, et al. Immediate delivery versus expectant monitoring for hypertensive disorders of pregnancy between 34 and 37 weeks of gestation (HYPITAT‐II): an open‐label, randomised controlled trial. Lancet 2015;385:2492‐501. - PubMed
-
- Broekhuijsen K, Baaren GJ, Pampus M, Sikkema M, Woiski M, Oudijk M, et al. Delivery versus expectant monitoring for late preterm hypertensive disorders of pregnancy (HYPITAT‐II): a multicenter, open label, randomized controlled trial. American Journal of Obstetrics and Gynecology 2014;210(1 Suppl):S2.
-
- Langenveld J, Broekhuijsen K, Baaren GJ, Pampus MG, Kaam AH, Groen H, et al. Induction of labour versus expectant monitoring for gestational hypertension or mild pre‐eclampsia between 34 and 37 weeks' gestation (HYPITAT‐II): A multicentre, open‐label randomised controlled trial. BMC Pregnancy and Childbirth 2011;11:50. - PMC - PubMed
Hamed 2014 {published data only}
-
- Hamed HO, Alsheeha MA, Abu‐Elhasan AM, Elmoniem AEA, Kamal MM. Pregnancy outcomes of expectant management of stable mild to moderate chronic hypertension as compared with planned delivery. International Journal of Gynecology and Obstetrics 2014;17:15‐20. - PubMed
Koopmans 2009 {published data only}
-
- Bijlenga D, Birnie E, Mol B, Bekedam D, Boer K, Drogtop A, et al. Health‐related quality of life after induction of labor or expectant management in pregnancy‐induced hypertension and pre‐eclampsia at term. Hypertension in Pregnancy 2008;27(4):518.
-
- Bijlenga D, Koopmans CM, Birnie E, Mol BWJ, Post JA, Bloemenkamp KW, et al. Health‐related quality of life after induction of labor versus expectant monitoring in gestational hypertension or preeclampsia at term. Hypertension in Pregnancy 2011;30(3):260‐74. - PubMed
-
- Hermes W, Koopmans CM, Pampus MG, Franx A, Bloemenkamp KW, Post J, et al. Induction of labour or expectant monitoring in hypertensive pregnancy disorders at term: do women's postpartum cardiovascular risk factors differ between the two strategies?. European Journal of Obstetrics, Gynecology, and Reproductive Biology 2013;171(1):30‐4. - PubMed
-
- Koopmans C, Ven den Berg P, Moll BW, Groen H, Willekes, Kwee A, et al. Pregnancy‐induced hypertension and preeclampsia after 36 weeks: induction of labour versus expectant monitoring. The HYPITAT trial. Hypertension in Pregnancy 2008;27(4):421.
Majeed 2014 {published data only}
-
- Majeed A, Kundu S, Singh P. Study on induction of labour versus expectant management in gestational hypertension or mild preeclampsia after 36 weeks of gestation. BJOG: an International Journal of Obstetrics and Gynaecology 2014;121(Suppl 2):118.
Owens 2014 {published data only}
-
- Martin JN, Owens MY, Thigpen B, Parrish MR, Keiser SD, Wallace K. Management of late preterm pregnancy complicated by mild preeclampsia: A prospective randomized trial. Pregnancy Hypertension 2012;2(3):180. - PubMed
-
- NCT00789919. Mild preeclampsia near term: deliver or deliberate?. clinicaltrials.gov/ct2/show/NCT00789919 Date first received: 12 November 2008.
-
- Owens MY, Thigpen B, Parrish MR, Keiser SD, Sawardecker S, Wallace K, et al. Management of preeclampsia when diagnosed between 34‐37 weeks gestation: deliver now or deliberate until 37 weeks?. Journal of the Mississippi State Medical Association 2014;55(7):208‐11. - PubMed
References to studies excluded from this review
Ramrakhyani 2001 {published data only}
-
- Ramrakhyani N, Sharma SK, Sankhla J, Sharma SK. Role of active management of pregnancy with hypertension in improving maternal and foetal outcome. Journal of the Association of Physicians of India 2001;49(1):Abstract no: 149.
Tukur 2007 {published data only}
-
- Tukur J, Umar NI, Khan N, Musa D. Comparison of emergency caesarean section to misoprostol induction for the delivery of antepartum eclamptic patients: a pilot study. Nigerian Journal of Medicine 2007;16(4):364‐7. - PubMed
References to ongoing studies
Shennan 2013 {published data only}
-
- ISRCTN01879376. PHOENIX ‐ Pre‐eclampsia in HOspital: Early iNductIon or eXpectant management. isrctn.com/ISRCTN01879376 Date first received: 20 November 2013.
Additional references
Abalos 2013
-
- Abalos E, Cuesta C, Grosso AL, Chou D, Say L. Global and regional estimates of preeclampsia and eclampsia: a systematic review. European Journal of Obstetrics, Gynecology, and Reproductive Biology 2013;170(1):1‐7. [doi: 10.1016/j.ejogrb.2013.05.005] - PubMed
ACOG Hypertension in Pregnancy 2013
-
- Roberts JM, August PA, Bakris G, Barton JR, Bernstein IM, Druzin M, et al. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstetrics and Gynecology 2013;122(5):1122‐31. - PubMed
ACOG No. 560 2013
-
- Committee Opinion No. 560. American College of Obstetricians and Gynaecologists. Medically indicated late‐preterm and early‐term deliveries. Obstetrics and Gynecology 2013; Vol. 121, issue 4:908‐10. - PubMed
August 2012
-
- August P, Sibai BM. Preeclampsia: Clinical features and diagnosis. www.uptodate.com/contents/preeclampsia‐clinical‐features‐and‐diagnosis (accessed 10 March 2014).
Barton 2001
-
- Barton JR, O'Brien JM, Bergauer NK, Jacques DL, Sibai BM. Mild gestational hypertension remote from term: progression and outcome. American Journal of Obstetrics and Gynecology 2001;184(5):979‐83. - PubMed
Belizan 1980
-
- Belizan JM, Villar J. The relationship between calcium intake and edema, proteinuria, and hypertension‐gestosis: an hypothesis. American Journal of Clinical Nutrition 1980;33(10):2202‐10. - PubMed
Boyle 2012
Bujold 2014
-
- Bujold E, Roberge S, Nicolaides KH. Low‐dose aspirin for prevention of adverse outcomes related to abnormal placentation. Prenatal Diagnosis 2014;34(7):642‐8. - PubMed
Churchill 2013
Davis 2007
-
- Davis GK, Mackenzie C, Brown MA, Homer CS, Holt J, McHugh L, et al. Predicting transformation from gestational hypertension to preeclampsia in clinical practice: a possible role for 24 hour ambulatory blood pressure monitoring. Hypertension in Pregnancy 2007;26(1):77‐87. - PubMed
De Regil 2011
Dietz 2012
-
- Dietz PM, Rizzo JH, England LJ, Callaghan WM, Vesco KK, Bruce FC, et al. Early term delivery and health care utilization in the first year of life. Journal of Pediatrics 2012;161(2):234‐9. - PubMed
Dolea 2003
-
- Dolea C, AbouZahr C. Global burden of hypertensive disorders of pregnancy in the year 2000. Evidence and Information for Policy (EIP), World Health Organization, Geneva, July 2003. www.who.int/healthinfo/statistics/bod_hypertensivedisordersofpregnancy.pdf (Accessed on December 12, 2012).
Duley 2009
-
- Duley L, Henderson‐Smart DJ, Walker GJA. Interventions for treating pre‐eclampsia and its consequences: generic protocol. Cochrane Database of Systematic Reviews 2009, Issue 2. [DOI: 10.1002/14651858.CD007756] - DOI
Higgins 2011
-
- Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Hofmeyr 2014
Hutcheon 2011
-
- Hutcheon JA, Lisonkova S, Joseph KS. Epidemiology of pre‐eclampsia and the other hypertensive disorders of pregnancy. Best Practice & Research. Clinical Obstetrics & Gynaecology 2011;25(4):391‐403. - PubMed
Khan 2006
-
- Khan KS, Wojdyla D, Say L, Gülmezoglu AM, Look PF. WHO analysis of causes of maternal death: systematic review. Lancet 2006;367(9516):1066‐74. - PubMed
Lowe 2014
-
- Lowe SA, Bowyer L, Lust K, McMahon LP, Morton MR, North RA, et al. Guideline for the Management of Hypertensive Disorders of Pregnancy. Society of Obstetric Medicine of Australia and New Zealand (SOMANZ) 2014. - PubMed
Magee 2008
-
- Magee LA, Helewa M, Moutquin JM, Dadelszen P, Hypertension Guideline Committee, Strategic Training Initiative in Research in the Reproductive Health Sciences (STIRRHS) Scholars. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. Journal of Obstetrics and Gynaecology Canada: JOGC 2008;30(3 Suppl):S1. - PubMed
Magee 2014
-
- Magee LA, Pels A, Helewa M, Rey E, Dadelszen P. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. Pregnancy Hypertension: An International Journal of Women's Cardiovascular Health 2014;4(2):105‐45. - PubMed
Magloire 2012
-
- Magloire L, Funai EF. Gestational hypertension. www.uptodate.com/contents/gestational‐hypertension (accessed 10 March 2014).
Maslow 2000
-
- Maslow AS, Sweeny AL. Elective induction of labor as a risk factor for cesarean delivery among low‐risk women at term. Obstetrics and Gynecology 2000;95(6 Pt 1):917‐22. - PubMed
Meher 2005
-
- Meher S, Duley L, Prevention of Pre‐eclampsia Cochrane Review Authors. Interventions for preventing pre‐eclampsia and its consequences: generic protocol. Cochrane Database of Systematic Reviews 2005, Issue 2. [DOI: 10.1002/14651858.CD005301] - DOI
NICE 2010
-
- National Collaborating Centre for Women’s and Children’s Health. Hypertension in Pregnancy: the Management of Hypertensive Disorders During Pregnancy. NICE Clinical Guideline 107. London: National Institute for Health and Clinical Excellence, August 2010.
Norwitz 2013
-
- Norwitz ER, Funai EF. Expectant management of severe preeclampsia. www.uptodate.com/contents/expectant‐management‐of‐severe‐preeclampsia (accessed 10 March 2014). - PubMed
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Saftlas 1990
-
- Saftlas AF, Olson DR, Franks AL, Atrash AK, Pokras R. Epidemiology of preeclampsia and eclampsia in the United States, 1979‐1986. American Journal of Obstetrics and Gynecology 1990;163(2):460‐5. - PubMed
Sibai 2005
-
- Sibai B, Dekker G, Kupferminc G. Pre‐eclampsia. Lancet 2005;365(9461):785‐99. - PubMed
Spong 2011
Steegers 2010
-
- Steegers EAP, Dadelszen P, Pijnenbong R. Pre‐eclampsia. Lancet 2010;376:631‐44. - PubMed
Tita 2009
Villar 2003
-
- Villar J, Say L, Gülmezoglu M, et al. Eclampsia and preeclampsia: a worldwide health problem for 2000 years. In: Critchley H, Maclean A, Poston L, Walker J editor(s). Pre‐eclampsia. London, England: RCOG Press, 2003:57‐72.
Wang 2004
-
- Wang ML, Dorer DJ, Fleming MP, Catlin EA. Clinical outcomes of near‐term infants. Pediatrics 2004;114(2):372‐6. - PubMed
WHO 2011
-
- World Health Organization. WHO Recommendations for Prevention and Treatment of Pre‐eclampsia and Eclampsia. Geneva: WHO, 2011. - PubMed
Wilmink 2010
-
- Wilmink FA, Hukkelhoven CW, Lunshof S, Mol BW, Post JA, Papatsonis DN. Neonatal outcome following elective cesarean section beyond 37 weeks of gestation: a 7‐year retrospective analysis of a national registry. American Journal of Obstetrics and Gynecology 2010;202(3):1‐8. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical