

Cash vs. food assistance to improve adherence to antiretroviral therapy among HIV-infected adults in Tanzania
- PMID: 28107221
- PMCID: PMC5342932
- DOI: 10.1097/QAD.0000000000001406
Cash vs. food assistance to improve adherence to antiretroviral therapy among HIV-infected adults in Tanzania
Abstract
Objective: We evaluated the effectiveness of short-term cash and food assistance to improve adherence to antiretroviral therapy (ART) and retention in care among people living with HIV in Tanzania.
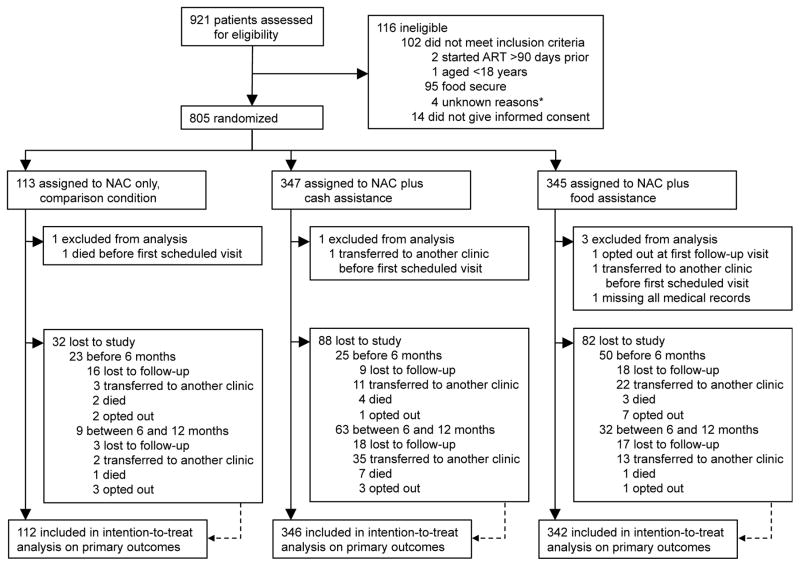
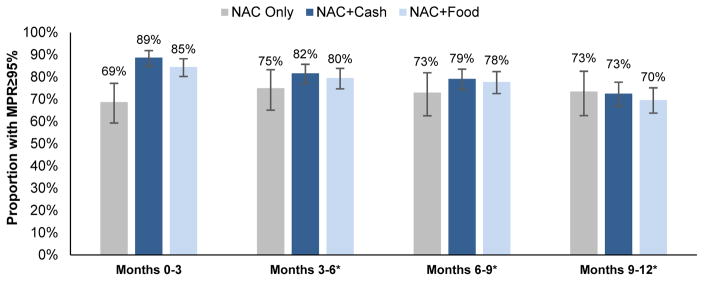
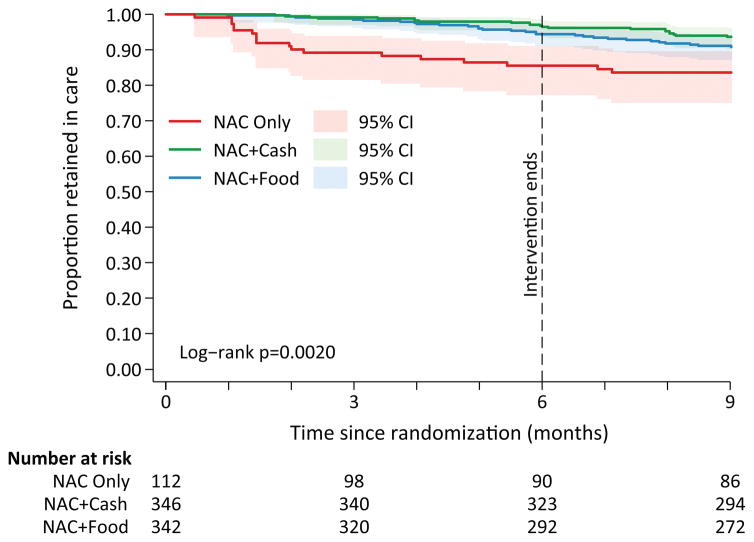
Methods: At three clinics, 805 participants were randomized to three groups in a 3 : 3 : 1 ratio, stratified by site : nutrition assessment and counseling (NAC) and cash transfers (∼$11/month, n = 347), NAC and food baskets (n = 345), and NAC-only (comparison group, n = 113, clinicaltrials.gov NCT01957917). Eligible people living with HIV were at least 18 years, initiated ART 90 days or less prior, and food insecure. Cash or food was provided for 6 or less consecutive months, conditional on visit attendance. The primary outcome was medication possession ratio (MPR ≥ 95%) at 6 months. Secondary outcomes were appointment attendance and loss to follow-up (LTFU) at 6 and 12 months.
Results: The primary intent-to-treat analysis included 800 participants. Achievement of MPR ≥ 95% at 6 months was higher in the NAC + cash group compared with NAC-only (85.0 vs. 63.4%), a 21.6 percentage point difference [95% confidence interval (CI): 9.8, 33.4, P < 0.01]. MPR ≥ 95% was also significantly higher in the NAC + food group vs. NAC-only (difference = 15.8, 95% CI: 3.8, 27.9, P < 0.01). When directly compared, MPR ≥ 95% was similar in the NAC + cash and NAC + food groups (difference = 5.7, 95% CI: -1.2, 12.7, P = 0.15). Compared with NAC-only, appointment attendance and LTFU were significantly higher in both the NAC + cash and NAC + food groups at 6 months. At 12 months, the effect of NAC + cash, but not NAC + food, on MPR ≥ 95% and retention was sustained.
Conclusion: Short-term conditional cash and food assistance improves ART possession and appointment attendance and reduces LTFU among food-insecure ART initiates in Tanzania.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- World Health Organization. Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. Geneva: 2015. - PubMed
-
- Paterson DL, Swindells S, Mohr J, Brester M, Vergis EN, Squier C, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21–30. - PubMed
-
- Bangsberg DR. Less than 95% adherence to nonnucleoside reverse-transcriptase inhibitor therapy can lead to viral suppression. Clin Infect Dis. 2006;43(7):939–941. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
