

Readmission and Late Mortality After Critical Illness in Childhood
- PMID: 28107264
- PMCID: PMC5336515
- DOI: 10.1097/PCC.0000000000001062
Readmission and Late Mortality After Critical Illness in Childhood
Abstract
Objectives: Little is known about the ongoing mortality risk and healthcare utilization among U.S. children after discharge from a hospitalization involving ICU care. We sought to understand risks for hospital readmission and trends in mortality during the year following ICU discharge.
Design: Retrospective observational cohort study.
Setting: This study was performed using administrative claims data from 2006-2013 obtained from the Truven Health Analytics MarketScan Database.
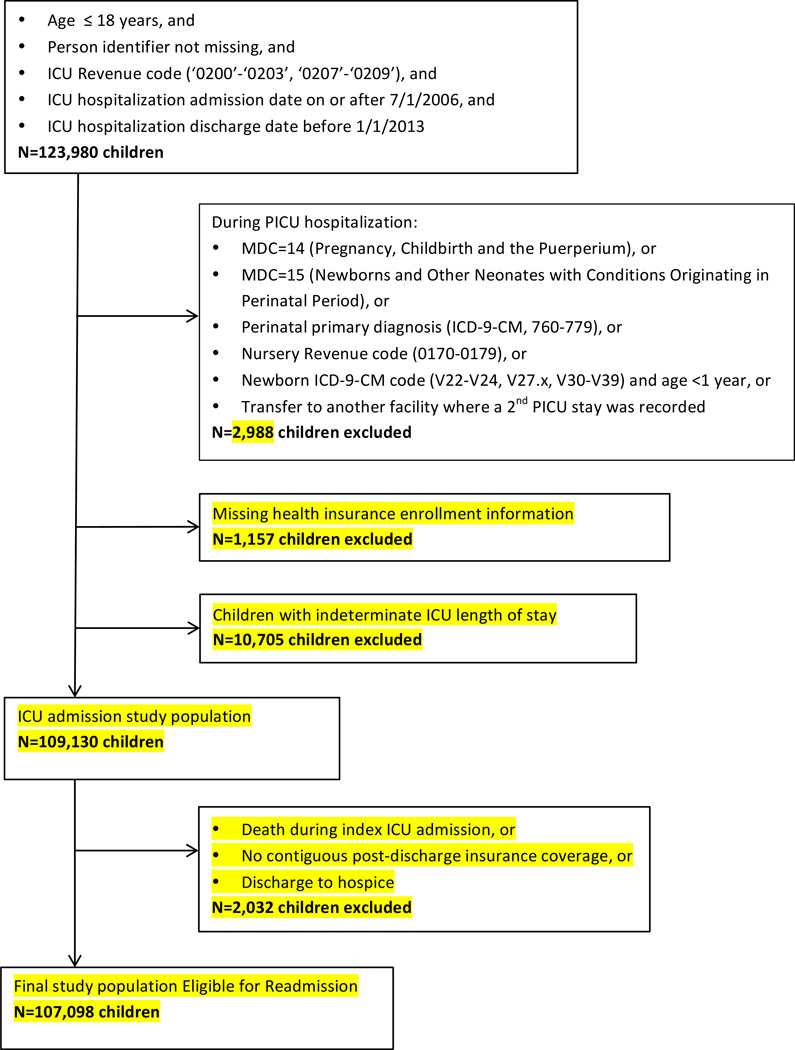
Subjects: We included all children in the dataset admitted to a U.S. ICU less than or equal to 18 years old.
Interventions: The primary outcome was nonelective readmission in the year following discharge. Risk of rehospitalization was determined using a Cox proportional hazards model.
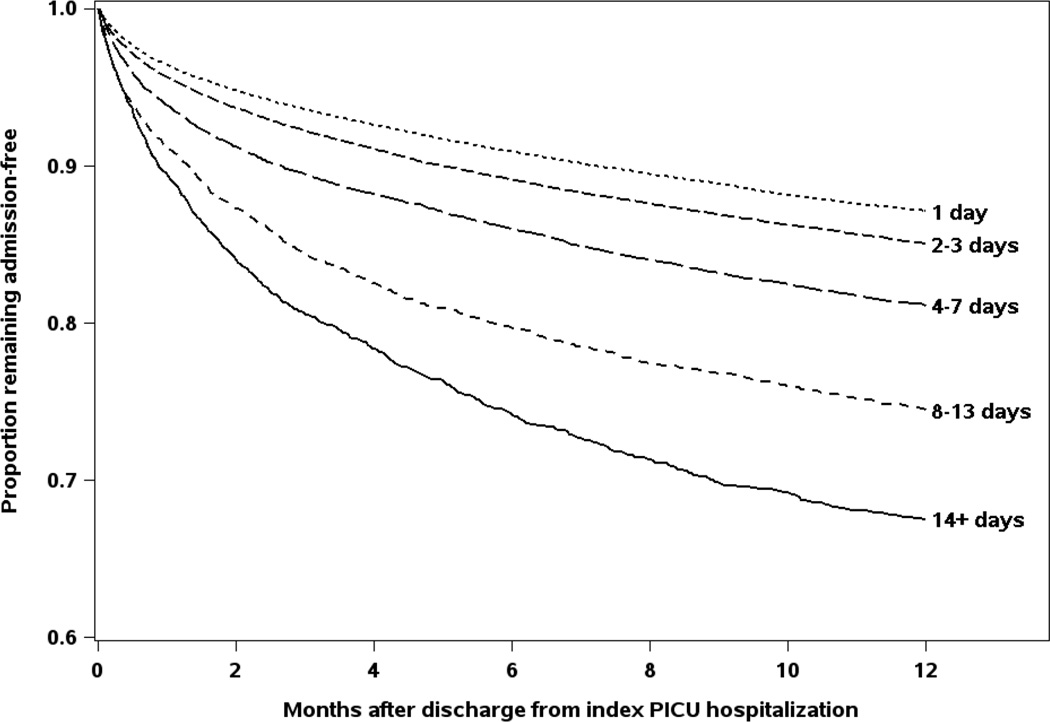
Measurements and main results: We identified 109,130 children with at least one ICU admission in the dataset. Over three quarters of the index ICU admissions (78.6%) had an ICU length of stay less than or equal to 3 days, and the overall index hospitalization mortality rate was 1.4%. In multivariate analysis, risk of nonelective readmission for children without cancer was higher with longer index ICU admission length of stay, younger age, and several chronic and acute conditions. By the end of the 1-year observation period, 36.0% of children with an index ICU length of stay greater than or equal to 14 days had been readmitted, compared with only 13.9% of children who had an index ICU length of stay equals to 1 day. Mortality in the year after ICU discharge was low overall (106 deaths per 10,000 person-years of observation) but was high among children with an initial index ICU admission length of stay greater than or equal to 14 days (599 deaths per 10,000 person-years).
Conclusions: Readmission after ICU care is common. Further research is needed to investigate the potentially modifiable factors affecting likelihood of readmissions after discharge from the ICU. Although late mortality was relatively uncommon overall, it was 10-fold higher in the year after ICU discharge than in the general U.S. pediatric population.
Conflict of interest statement
Figures
Comment in
-
I Think I Took Care of Him Last Time He Was Here.Pediatr Crit Care Med. 2017 Mar;18(3):290-291. doi: 10.1097/PCC.0000000000001066. Pediatr Crit Care Med. 2017. PMID: 28257373 No abstract available.
References
-
- de Oliveira CF, de Oliveira DS, Gottschald AF, et al. ACCM/PALS haemodynamic support guidelines for paediatric septic shock: an outcomes comparison with and without monitoring central venous oxygen saturation. Intensive Care Med. 2008;34(6):1065–1075. - PubMed
-
- Tilford JM, Roberson PK, Lensing S, Fiser DH. Improvement in pediatric critical care outcomes. Crit Care Med. 2000;28(2):601–603. - PubMed
-
- Alkandari O, Eddington KA, Hyder A, et al. Acute kidney injury is an independent risk factor for pediatric intensive care unit mortality, longer length of stay and prolonged mechanical ventilation in critically ill children: a two-center retrospective cohort study. Crit Care. 2011;15(3):R146. - PMC - PubMed
-
- Tilford JM, Simpson PM, Green JW, Lensing S, Fiser DH. Volume-outcome relationships in pediatric intensive care units. Pediatrics. 2000;106(2 Pt 1):289–294. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
