

Recent advances in understanding clonal haematopoiesis in aplastic anaemia
- PMID: 28107566
- PMCID: PMC5435524
- DOI: 10.1111/bjh.14510
Recent advances in understanding clonal haematopoiesis in aplastic anaemia
Abstract
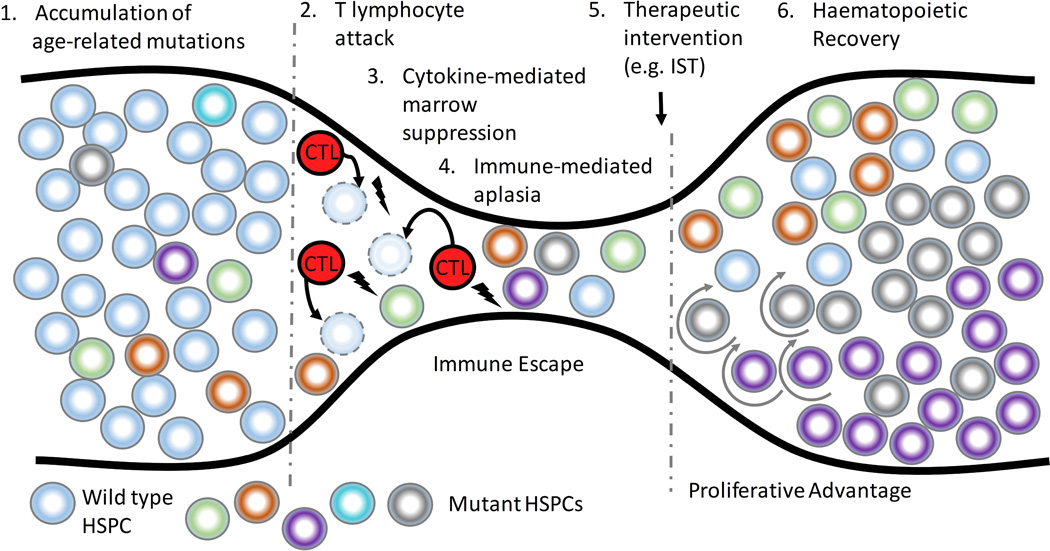
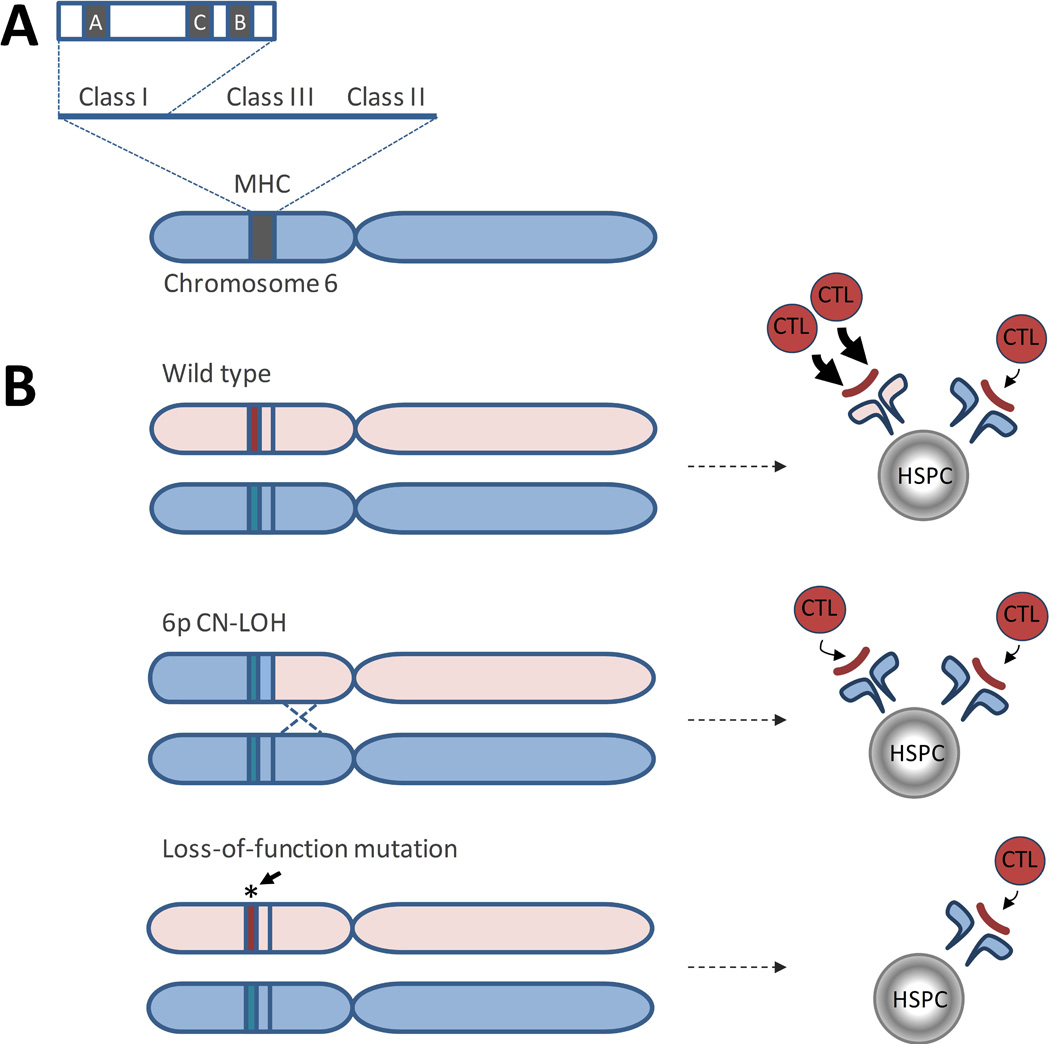
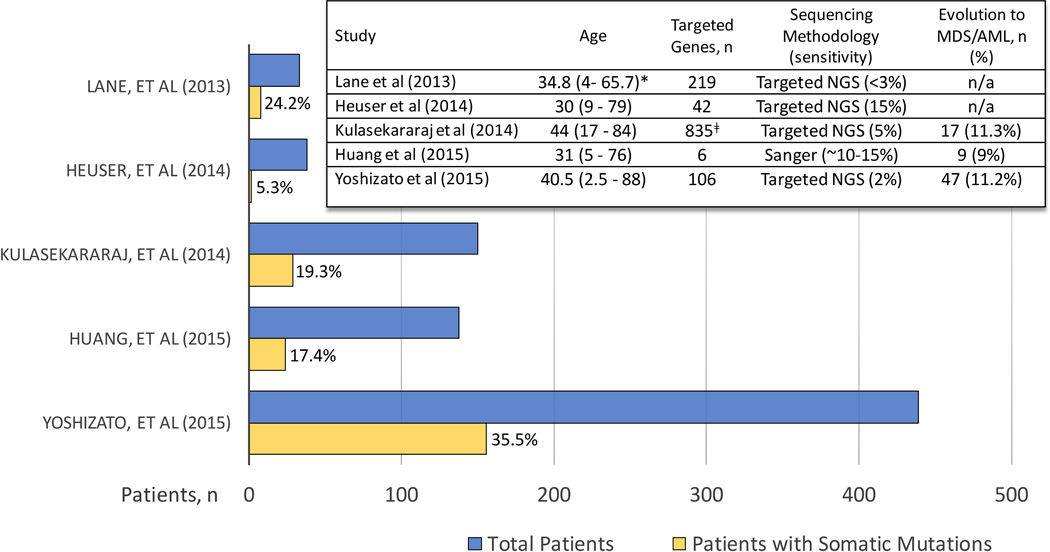
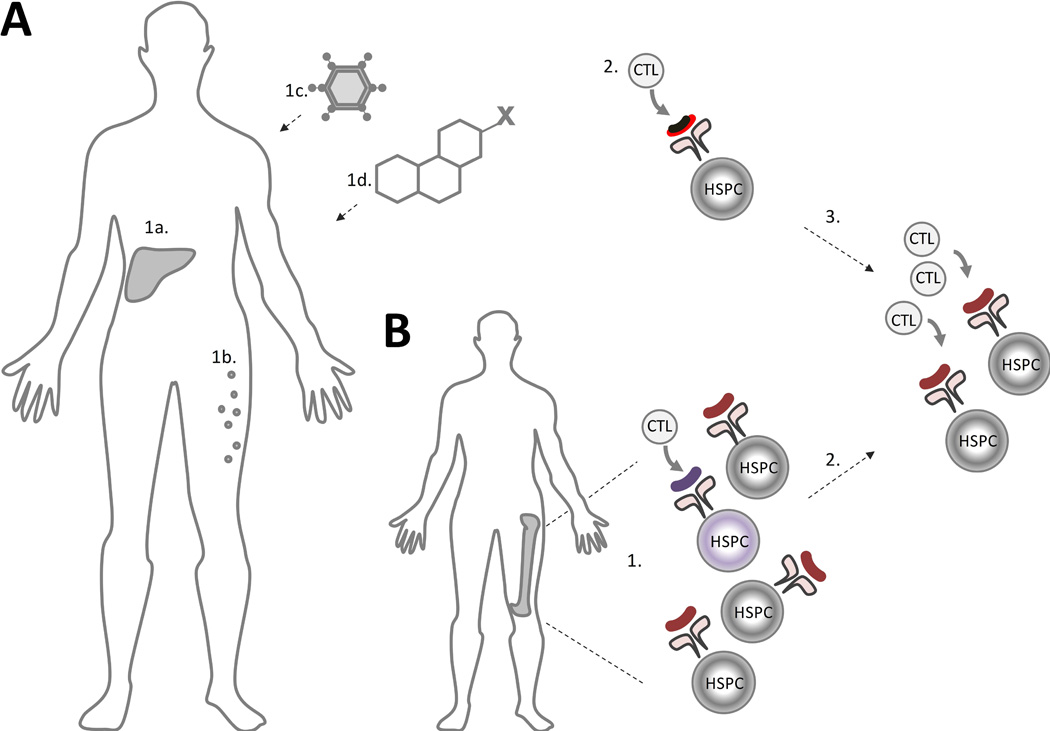
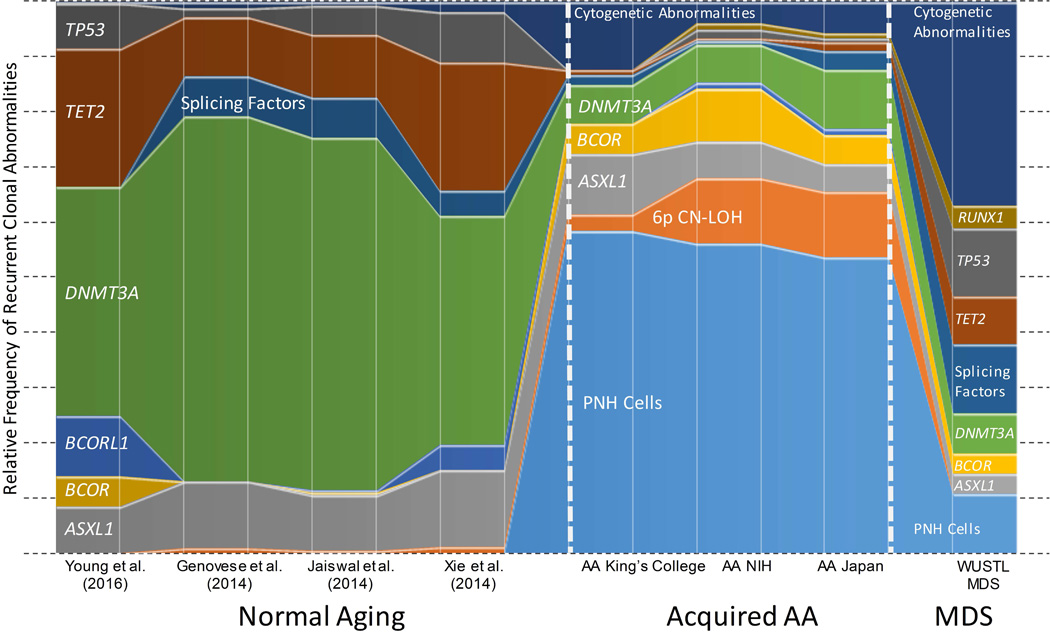
Acquired aplastic anaemia (AA) is an immune-mediated bone marrow failure disorder inextricably linked to clonal haematopoiesis. The majority of AA patients have somatic mutations and/or structural chromosomal abnormalities detected as early as at diagnosis. In contrast to other conditions linked to clonal haematopoiesis, the clonal signature of AA reflects its immune pathophysiology. The most common alterations are clonal expansions of cells lacking glycophosphotidylinositol-anchored proteins, loss of human leucocyte antigen alleles, and mutations in BCOR/BCORL1, ASXL1 and DNMT3A. Here, we present the current knowledge of clonal haematopoiesis in AA as it relates to aging, inherited bone marrow failure, and the grey-zone overlap of AA and myelodysplastic syndrome (MDS). We conclude by discussing the significance of clonal haematopoiesis both for improved diagnosis of AA, as well as for a more precise, personalized approach to prognostication of outcomes and therapy choices.
Keywords: CHIP; MDS; aplastic anaemia; bone marrow failure; clonal haematopoiesis.
© 2017 John Wiley & Sons Ltd.
Conflict of interest statement
Figures
References
-
- Abkowitz JL, Catlin SN, McCallie MT, Guttorp P. Evidence that the number of hematopoietic stem cells per animal is conserved in mammals. Blood. 2002;100:2665–2667. - PubMed
-
- Babushok DV, Xie HM, Roth JJ, Perdigones N, Olson TS, Cockroft JD, Gai X, Perin JC, Li Y, Paessler ME, Hakonarson H, Podsakoff GM, Mason PJ, Biegel JA, Bessler M. Single nucleotide polymorphism array analysis of bone marrow failure patients reveals characteristic patterns of genetic changes. British journal of haematology. 2014;164:73–82. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
