

Effects of mineralocorticoid receptor antagonists on the progression of diabetic nephropathy
- PMID: 28107779
- PMCID: PMC5497036
- DOI: 10.1111/jdi.12629
Effects of mineralocorticoid receptor antagonists on the progression of diabetic nephropathy
Abstract
Aims/introduction: We aimed to evaluate the potential benefits and adverse effects of adding a mineralocorticoid receptor antagonist (MRA) to angiotensin-converting enzyme inhibitors (ACEI) and/or angiotensin receptor blockers (ARB), as standard treatment in patients with diabetic nephropathy.
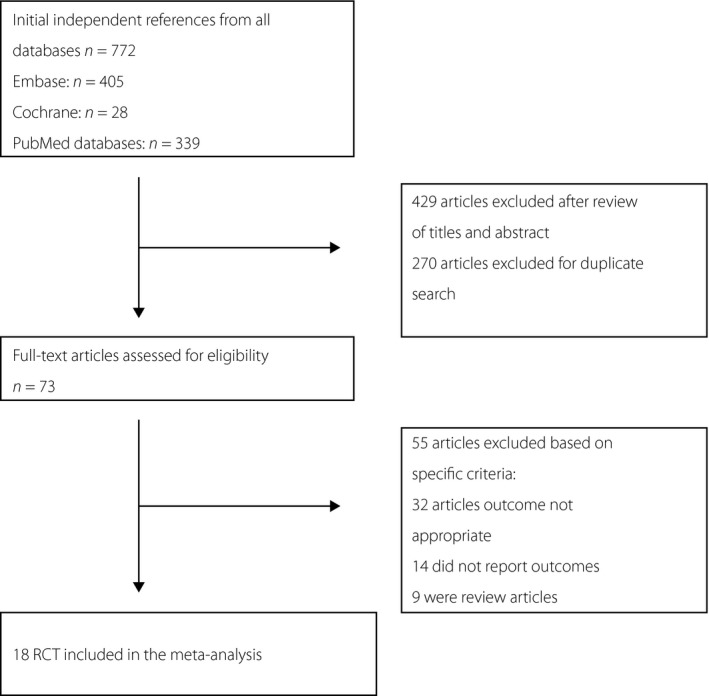
Materials and methods: We scanned the Embase, PubMed and Cochrane Central Register of Controlled Trials databases for human clinical trials published in English until June 2016, evaluating renal outcomes in patients with diabetic nephropathy.
Results: A total of 18 randomized controlled trials involving 1,786 patients were included. Compared with ACEI/ARB alone, co-administration of MRA and ACEI/ARB significantly reduced urinary albumin excretion and the urinary albumin-creatinine ratio (mean difference -69.38, 95% confidence intervals -103.53 to -35.22, P < 0.0001; mean difference -215.74, 95% confidence intervals -409.22 to -22.26, P = 0.03, respectively). A decrease of blood pressure was also found in the co-administration of MRA and ACEI/ARB groups. However, we did not observe any improvement in the glomerular filtration rate. There was a significant increase in the risk of hyperkalemia on the addition of MRA to ACEI/ARB treatment (relative risk 3.74, 95% confidence intervals 2.30-6.09, P < 0.00001).
Conclusions: These findings suggest that co-administration of MRA and ACEI/ARB has beneficial effects on renal outcomes with increasing the incidence of hyperkalemia.
Keywords: Diabetic nephropathy; Meta- analysis; Mineralocorticoid receptor antagonist.
© 2017 The Authors. Journal of Diabetes Investigation published by Asian Association for the Study of Diabetes (AASD) and John Wiley & Sons Australia, Ltd.
Figures






References
-
- Mima A. Diabetic nephropathy: protective factors and a new therapeutic paradigm. J Diabetes Complications 2013; 27: 526–530. - PubMed
-
- Mavrakanas TA, Gariani K, Martin PY. Mineralocorticoid receptor blockade in addition to angiotensin converting enzyme inhibitor or angiotensin II receptor blocker treatment: an emerging paradigm in diabetic nephropathy: a systematic review. Eur J Intern Med 2014; 25: 173–176. - PubMed
-
- Lian M, Hewitson TD, Wigg B, et al Long‐term mineralocorticoid receptor blockade ameliorates progression of experimental diabetic renal disease. Nephrol Dial Transplant 2012; 27: 906–912. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
