

"Unforgettable" - a pictorial essay on anatomy and pathology of the hippocampus
- PMID: 28108955
- PMCID: PMC5359145
- DOI: 10.1007/s13244-016-0541-2
"Unforgettable" - a pictorial essay on anatomy and pathology of the hippocampus
Abstract
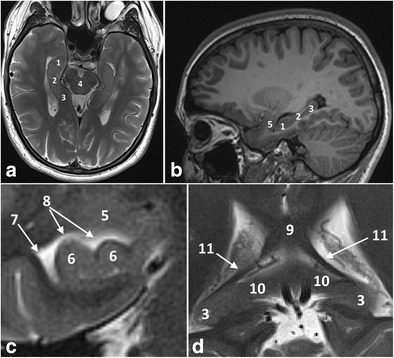
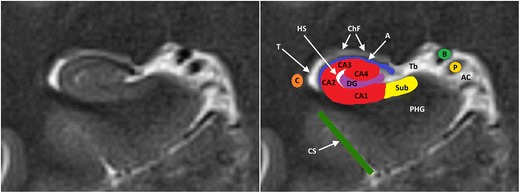
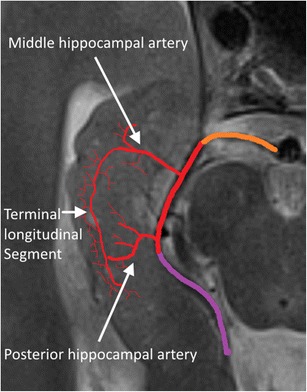
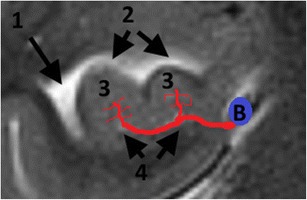
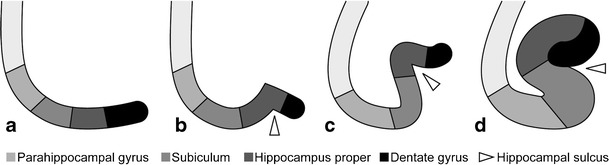
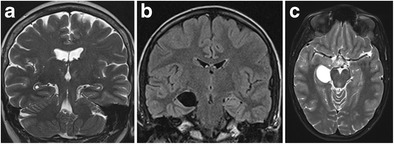
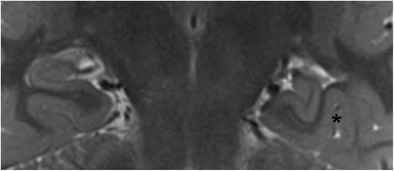
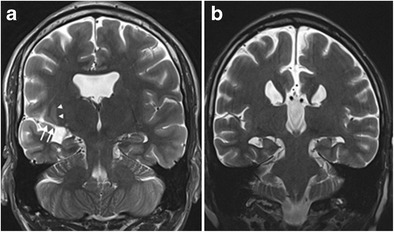
The hippocampus is a small but complex anatomical structure that plays an important role in spatial and episodic memory. The hippocampus can be affected by a wide range of congenital variants and degenerative, inflammatory, vascular, tumoral and toxic-metabolic pathologies. Magnetic resonance imaging is the preferred imaging technique for evaluating the hippocampus. The main indications requiring tailored imaging sequences of the hippocampus are medically refractory epilepsy and dementia. The purpose of this pictorial review is threefold: (1) to review the normal anatomy of the hippocampus on MRI; (2) to discuss the optimal imaging strategy for the evaluation of the hippocampus; and (3) to present a pictorial overview of the most common anatomic variants and pathologic conditions affecting the hippocampus.
Teaching points: • Knowledge of normal hippocampal anatomy helps recognize anatomic variants and hippocampal pathology. • Refractory epilepsy and dementia are the main indications requiring dedicated hippocampal imaging. • Pathologic conditions centered in and around the hippocampus often have similar imaging features. • Clinical information is often necessary to come to a correct diagnosis or an apt differential.
Keywords: Dementia; Epilepsy; Herpes simplex encephalitis; Hippocampus; MRI.
Conflict of interest statement
Martin Wiesmann has the following disclosures:
• Grants: Stryker Neurovascular. Siemens Healthcare
• Personal fees: Stryker Neurovascular. Silkroad Medical. Siemens Healthcare. Bracco
• Non-financial support: Codman Neurovascular. Covidien. Abbott. St. Jude Medical. Phenox. Penumbra. Microvention/Terumo. B. Braun. Bayer. Acandis. ab medica
The other authors have nothing to disclose.
The article received no grants or funding.
Figures

References
-
- Duvernoy HM. The Human Hippocampus: Functional Anatomy, Vascularization and Serial Sections with MRI. 3. Berlin: Springer Verlag; 2005.
-
- von Bechterew W. Demonstration eines Gehirns mit Zerstörung der vorderen und inneren Theile der Himrinde beider Schlafenlappen. Neurologisch Zentralbl. 1900;19:990–999.
-
- Barkhof F, Fox NC, Bastos-Leite AJ, Scheltens P. Neuroimaging in dementia. Berlin Heidelberg: Springer-Verlag; 2011.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
