

Effectiveness and cost-effectiveness of a guided Internet- and mobile-based intervention for the indicated prevention of major depression in patients with chronic back pain-study protocol of the PROD-BP multicenter pragmatic RCT
- PMID: 28109247
- PMCID: PMC5251328
- DOI: 10.1186/s12888-017-1193-6
Effectiveness and cost-effectiveness of a guided Internet- and mobile-based intervention for the indicated prevention of major depression in patients with chronic back pain-study protocol of the PROD-BP multicenter pragmatic RCT
Abstract
Background: Reducing the disease burden of major depressive disorder (MDD) is of major public health relevance. The prevention of depression is regarded as one possible approach to reach this goal. People with multiple risk factors for MDD such as chronic back pain and subthreshold depressive symptoms may benefit most from preventive measures. The Internet as intervention setting allows for scaling up preventive interventions on a public mental health level.
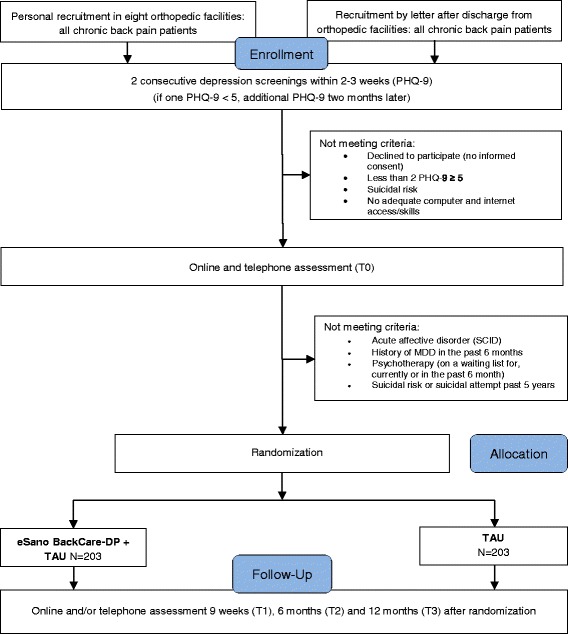
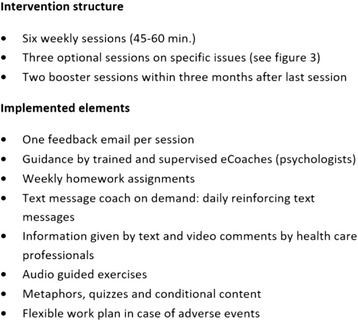
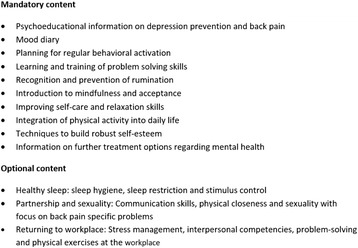
Methods: This study is a multicenter pragmatic randomized controlled trial (RCT) of parallel design aiming to investigate the (cost-) effectiveness of an Internet- and mobile-based intervention (IMI) for the prevention of depression in chronic back pain patients (PROD-BP) with subthreshold depressive symptoms. eSano BackCare-DP is a guided, chronic back pain-specific depression prevention intervention based on cognitive behavioral therapy (CBT) principles comprising six weekly plus three optional modules and two booster sessions after completion of the intervention. Trained psychologists provide guidance by sending feedback messages after each module. A total of 406 patients with chronic back pain and without a depressive disorder at baseline will be recruited following orthopedic rehabilitation care and allocated to either intervention or treatment-as-usual (TAU). Primary patient-relevant endpoint of the trial is the time to onset of MDD measured by the telephone-administered Structured Clinical Interview for DSM (SCID) at baseline and 1-year post-randomization. Key secondary outcomes are health-related quality of life, depression severity, pain intensity, pain-related disability, ability to work, intervention satisfaction and adherence as well as side effects of the intervention. Online assessments take place at baseline and 9 weeks as well as 6 and 12 months post-randomization. Cox regression survival analysis will be conducted to estimate hazard ratio at 12-month follow-up. Moreover, an economic analysis will be conducted from a societal and public health perspective.
Discussion: This is the first study examining an IMI for depression prevention in a sample of chronic pain patients. If this implementation of a depression prevention IMI into orthopedic aftercare proves effective, the intervention could be integrated into routine care with minimal costs and extended for use with other chronic diseases. Results will have implications for researchers, health care providers and public health policy makers.
Trial registration: The trial is registered at the WHO International Clinical Trials Registry Platform via the German Clinical Studies Trial Register (DRKS): DRKS00007960 . Registered 12 August 2015.
Keywords: CBT; Chronic back pain; Economic evaluation; Effectiveness; Internet and mobile based; Major depression; Prevention; RCT; eHealth.
Figures
References
-
- World Health Organization . The global burden of disease: 2004 update [Internet] Geneva: WHO Press; 2008.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
