

Common and uncommon neurological manifestations of neuroborreliosis leading to hospitalization
- PMID: 28109263
- PMCID: PMC5251276
- DOI: 10.1186/s12879-016-2112-z
Common and uncommon neurological manifestations of neuroborreliosis leading to hospitalization
Abstract
Background: Neuroborreliosis represents a relevant infectious disease and can cause a variety of neurological manifestations. Different stages and syndromes are described and atypical symptoms can result in diagnostic delay or misdiagnosis. The aim of this retrospective study was to define the pivotal neurological deficits in patients with neuroborreliosis that were the reason for admission in a hospital.
Methods: We retrospectively evaluated data of patients with neuroborreliosis. Only patients who fulfilled the diagnostic criteria of an intrathecal antibody production against Borrelia burgdorferi were included in the study.
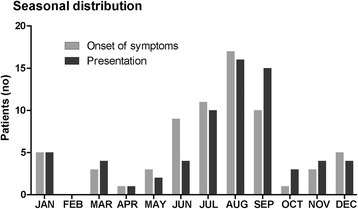
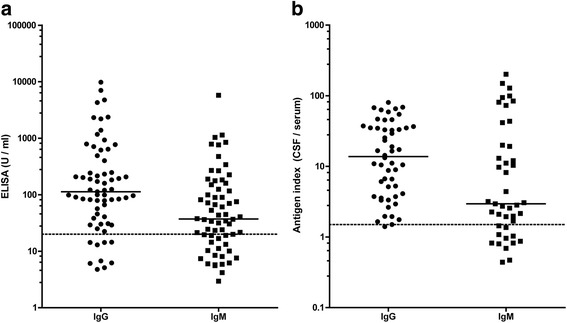
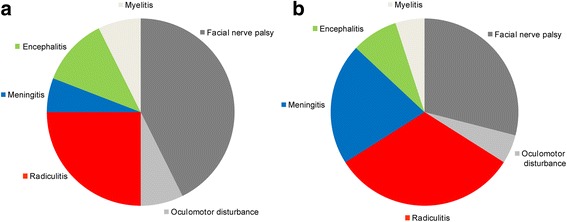
Results: Sixty-eight patients were identified with neuroborreliosis. Cranial nerve palsy was the most frequent deficit (50%) which caused admission to a hospital followed by painful radiculitis (25%), encephalitis (12%), myelitis (7%), and meningitis/headache (6%). In patients with a combination of deficits, back pain was the first symptom, followed by headache, and finally by cranial nerve palsy. Indeed, signs of meningitis were often found in patients with neuroborreliosis, but usually did not cause admission to a hospital. Unusual cases included patients with sudden onset paresis that were initially misdiagnosed as stroke and one patient with acute delirium. Cerebrospinal fluid (CSF) analysis revealed typical changes including elevated CSF cell count in all but one patient, a blood-CSF barrier dysfunction (87%), CSF oligoclonal bands (90%), and quantitative intrathecal synthesis of immunoglobulins (IgM in 74%, IgG in 47%, and IgA in 32% patients). Importantly, 6% of patients did not show Borrelia specific antibodies in the blood.
Conclusion: In conclusion, the majority of patients presented with typical neurological deficits. However, unusual cases such as acute delirium indicate that neuroborreliosis has to be considered in a wide spectrum of neurological diseases. CSF analysis is essential for a reliable diagnosis of neuroborreliosis.
Figures
Similar articles
-
[Clinical forms of neuroborreliosis among hospitalized patients in the years 2000-2005].Pol Merkur Lekarski. 2007 Aug;23(134):103-6. Pol Merkur Lekarski. 2007. PMID: 18044338 Polish.
-
Uncommon manifestations of neuroborreliosis in children.Eur J Paediatr Neurol. 2010 May;14(3):274-7. doi: 10.1016/j.ejpn.2009.08.003. Epub 2009 Sep 12. Eur J Paediatr Neurol. 2010. PMID: 19748808
-
Lyme neuroborreliosis in cases of non-specific neurological symptoms.Tidsskr Nor Laegeforen. 2017 Jan 24;137(2):101-104. doi: 10.4045/tidsskr.15.1115. eCollection 2017 Jan. Tidsskr Nor Laegeforen. 2017. PMID: 28127071 English, Norwegian.
-
[Pain and neuroborreliosis].MMW Fortschr Med. 2004 Jul 22;146(29-30):38-41. MMW Fortschr Med. 2004. PMID: 15540558 Review. German.
-
Clinical aspects of neuroborreliosis and post-Lyme disease syndrome in adult patients.Int J Med Microbiol. 2006 May;296 Suppl 40:11-6. doi: 10.1016/j.ijmm.2005.12.003. Epub 2006 Mar 9. Int J Med Microbiol. 2006. PMID: 16524775 Review.
Cited by
-
The Usefulness of Two CXCL13 Assays on Cerebrospinal Fluid for the Diagnosis of Lyme Neuroborreliosis: a Retrospective Study in a Routine Clinical Setting.J Clin Microbiol. 2021 Aug 18;59(9):e0025521. doi: 10.1128/JCM.00255-21. Epub 2021 Aug 18. J Clin Microbiol. 2021. PMID: 34132584 Free PMC article.
-
Incidence of notified Lyme borreliosis in Germany, 2013-2017.Sci Rep. 2018 Oct 8;8(1):14976. doi: 10.1038/s41598-018-33136-0. Sci Rep. 2018. PMID: 30297731 Free PMC article.
-
Impact of the McDonald Criteria 2017 on Early Diagnosis of Relapsing-Remitting Multiple Sclerosis.Front Neurol. 2019 Mar 15;10:188. doi: 10.3389/fneur.2019.00188. eCollection 2019. Front Neurol. 2019. PMID: 30930829 Free PMC article. Review.
-
Case report: Successive ipsilateral and contralateral laryngeal nerve palsy as probable manifestation of neuroborreliosis.Heliyon. 2023 Oct 11;9(10):e20869. doi: 10.1016/j.heliyon.2023.e20869. eCollection 2023 Oct. Heliyon. 2023. PMID: 37876487 Free PMC article.
-
Clinical and epidemiological features of Lyme neuroborreliosis in adults and factors associated with polyradiculitis, facial palsy and encephalitis or myelitis.Sci Rep. 2023 Nov 14;13(1):19881. doi: 10.1038/s41598-023-47312-4. Sci Rep. 2023. PMID: 37964035 Free PMC article.
References
-
- Zajkowska J, Czupryna P, Kusmierczyk J, Ciemerych A, Ciemerych M, Kondrusik M, Pancewicz S, Grygorczuk S, Hermanowska-Szpakowicz T. Clinical forms of neuroborreliosis--the analysis of patients diagnosed in department of infectious diseases and neuroinfection medical academy in Bialystok between 2000–2005. Przegl Epidemiol. 2007;61(1):59–65. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
