

Age-Specific Profiles of Antibody Responses against Respiratory Syncytial Virus Infection
- PMID: 28111238
- PMCID: PMC5474434
- DOI: 10.1016/j.ebiom.2017.01.014
Age-Specific Profiles of Antibody Responses against Respiratory Syncytial Virus Infection
Abstract
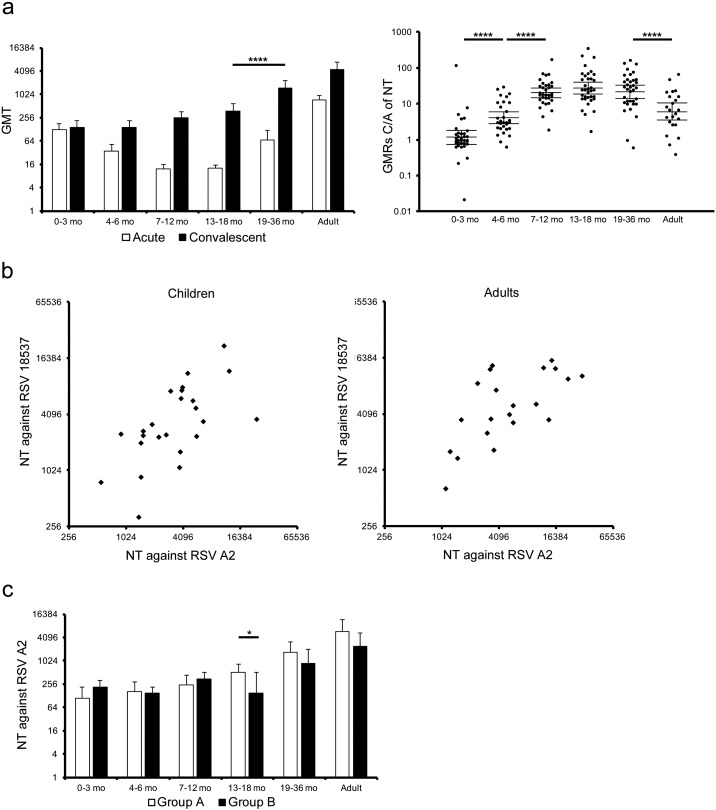
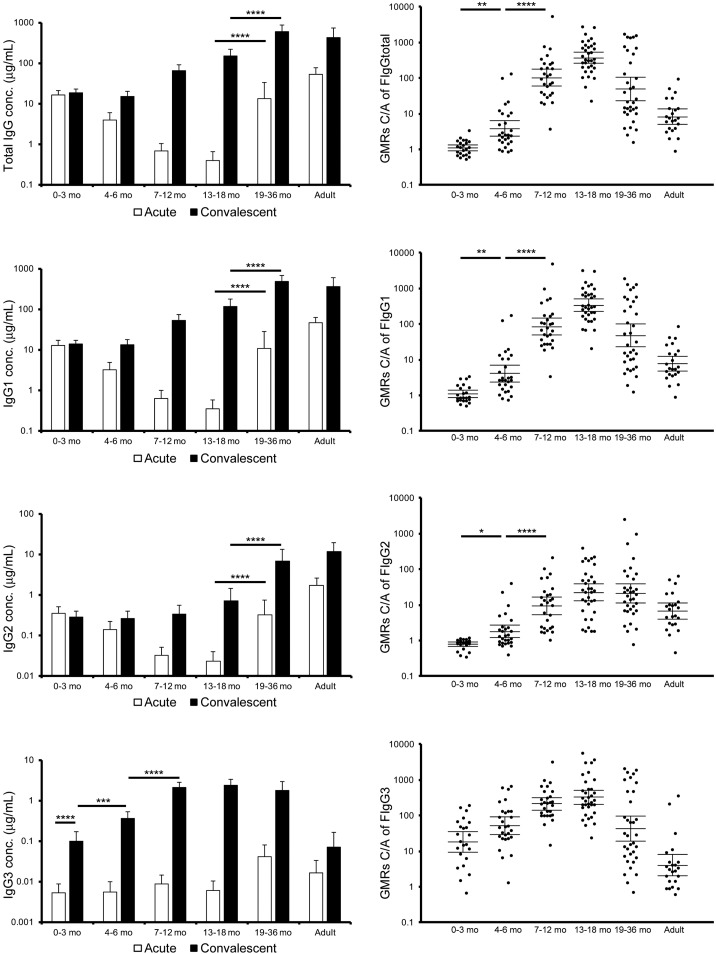
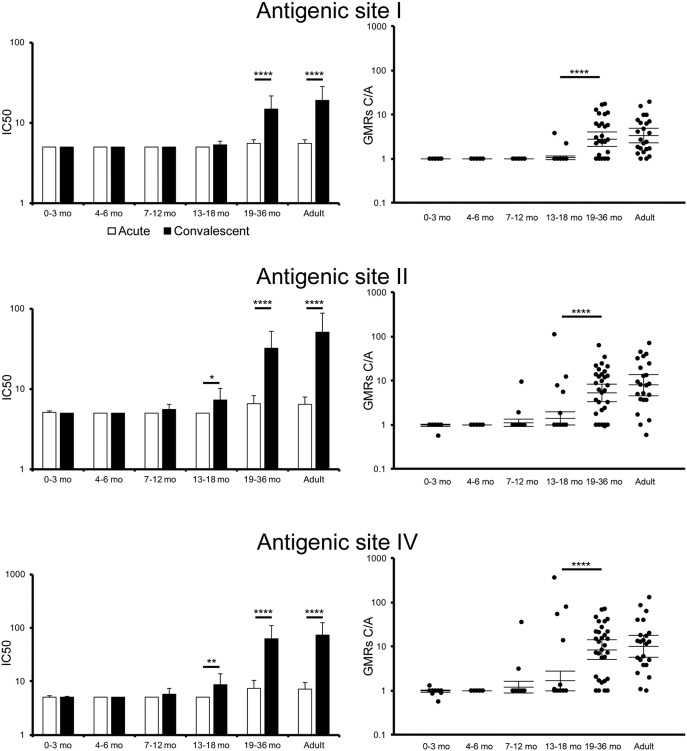
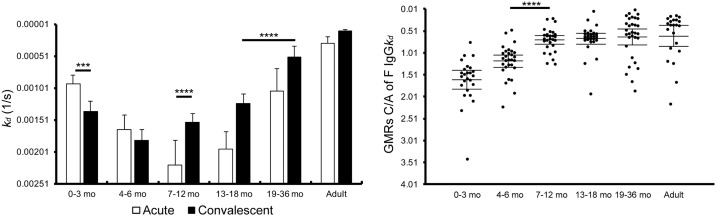
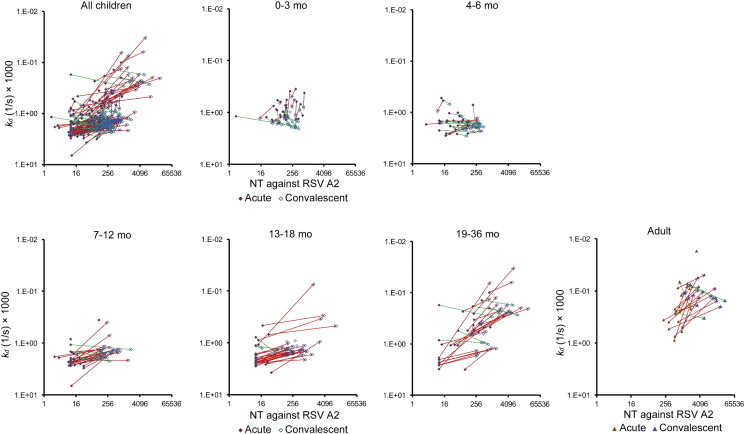
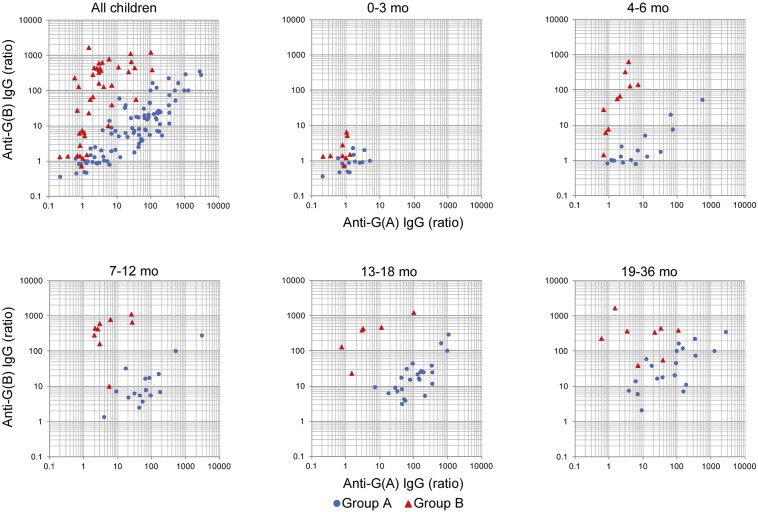
Respiratory syncytial virus (RSV) is one of the most prevalent causative agents of lower respiratory tract infections worldwide, especially in infants around 3 to 4months old. Infants at such a young age have maternally-transferred passive antibodies against RSV but do not have active immune systems efficient enough for the control of RSV infection. In order to elucidate age-specific profiles of immune responses against RSV protection, antibody responses were examined by using blood samples in both acute and convalescent phases obtained from child patients and adult patients. In addition to the serum neutralization activity, antibody responses to the RSV fusion protein (F protein) were dissected by analyzing levels of total IgG, IgG subclasses, the binding stability, and the levels of antibody for the neutralization epitopes. It was suggested that children's antibody responses against RSV are matured over months and years in at least 5 stages based on 1) levels of the neutralization titer and IgG3 for F protein in the convalescent phase, 2) geometric mean ratios of the neutralization titers and levels of IgG1 and IgG2 for F protein in the convalescent phase compared to those levels in the acute phase, 3) the affinity maturation of IgG for F protein and the cross reactivity of IgG for RSV glycoproteins of groups A and B, 4) levels of neutralization epitope-specific IgG, and 5) augmentation of overall antibody responses due to repetitive RSV infection.
Keywords: F protein; IgG3; Palivizumab-like neutralization antibody; RSV.
Copyright © 2017 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
IgG3 Snitcher of RSV Infections in the Very Young.EBioMedicine. 2017 Feb;16:10-11. doi: 10.1016/j.ebiom.2017.01.039. Epub 2017 Jan 30. EBioMedicine. 2017. PMID: 28159571 Free PMC article. No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
