

doi: 10.1007/s10388-016-0556-2.
Epub 2016 Nov 10.
Japanese Classification of Esophageal Cancer, 11th Edition: part II and III
- PMID: 28111536
- PMCID: PMC5222925
- DOI: 10.1007/s10388-016-0556-2
Item in Clipboard
Japanese Classification of Esophageal Cancer, 11th Edition: part II and III
Esophagus.
2017.
No abstract available
Figures
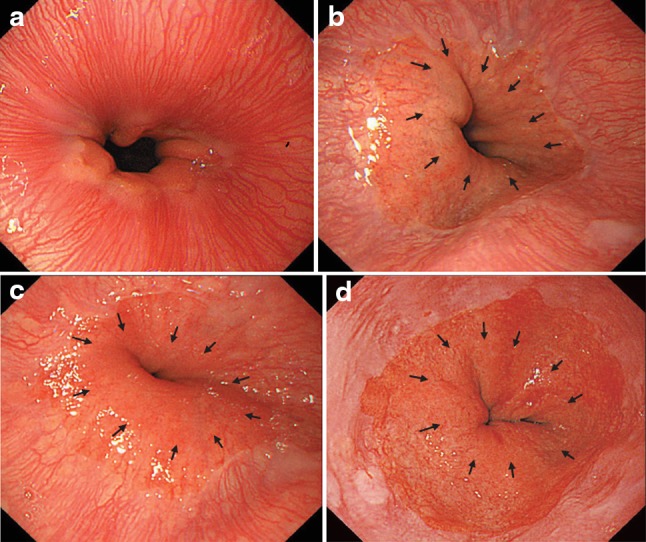
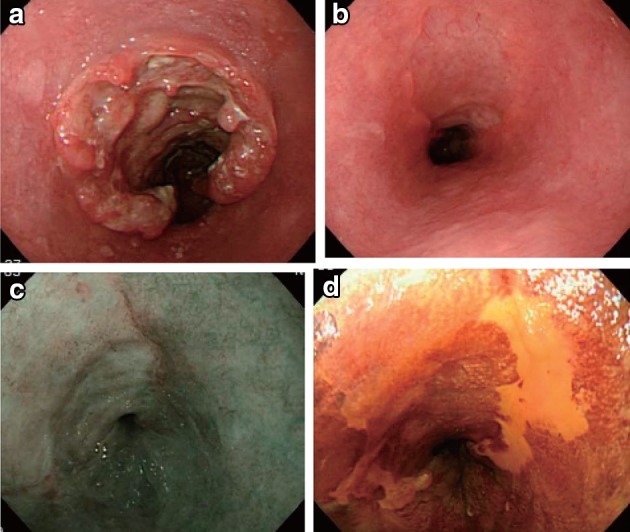
a The lower margin of the palisading small vessels and the oral margin of the longitudinal folds of the greater curvature of the stomach are both clearly visible and coincident at the same level. In such cases, this site of coincidence is defined as the EGJ and is nearly identical to the SCJ. b The lower margin of the palisading small vessels and the oral margin of the longitudinal folds of the greater curvature of the stomach are both clearly visible and coincident at the same level. In such cases, this site of coincidence is defined as the EGJ (black arrows). The gap between the SCJ and the EGJ is diagnosed as Barrett esophagus. c The palisading small vessels are visible, but the longitudinal folds are unclear. The lower margin of the palisading small vessels is defined as the EGJ (black arrows). The gap between the SCJ and the EGJ is diagnosed as Barrett esophagus. d The longitudinal folds are visible, but the lower margin of the palisading vessels is unclear. The upper oral margin of the longitudinal fold is defined as the EGJ (black arrows). The gap between the SCJ and the EGJ is diagnosed as Barrett esophagus
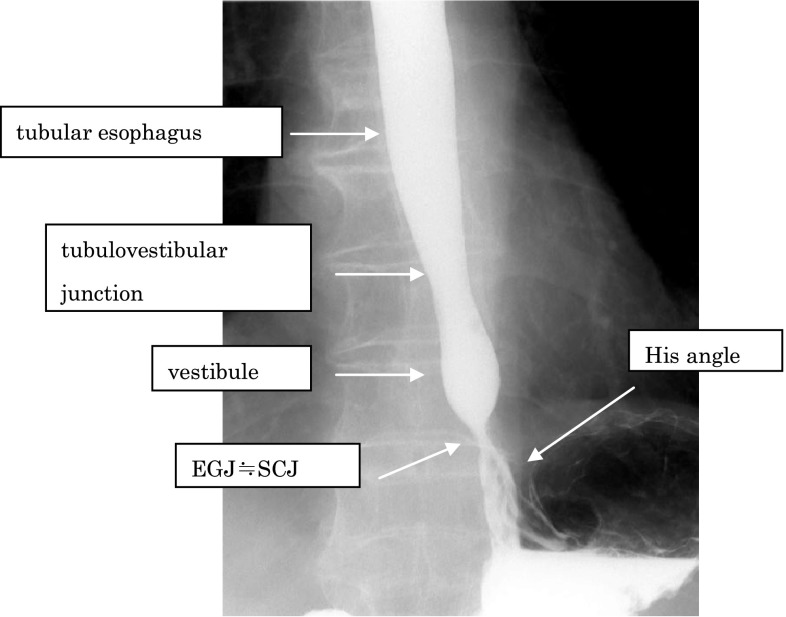
Barium contrast image of a normal EGJ
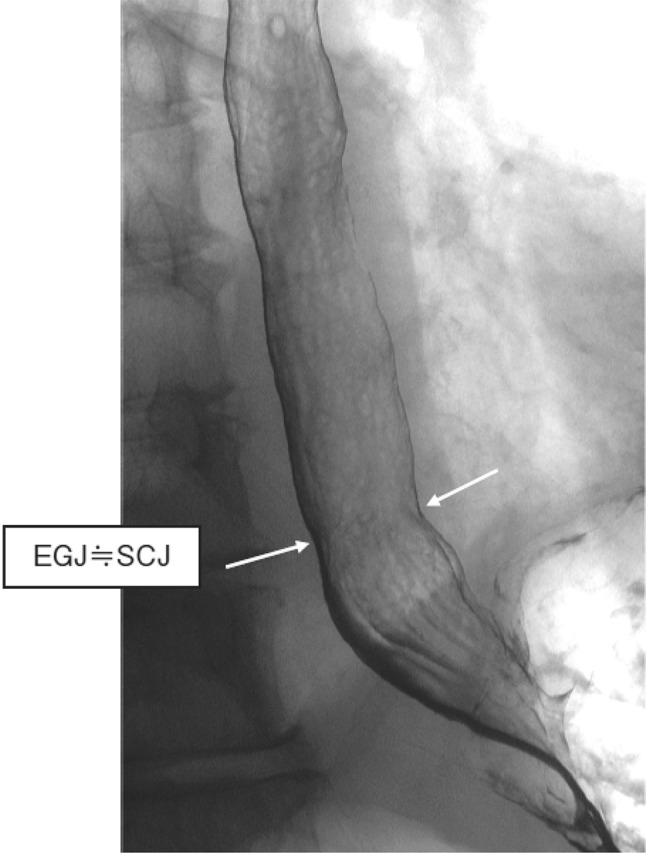
Barium contrast image of the EGJ in a subject with a hiatal hernia
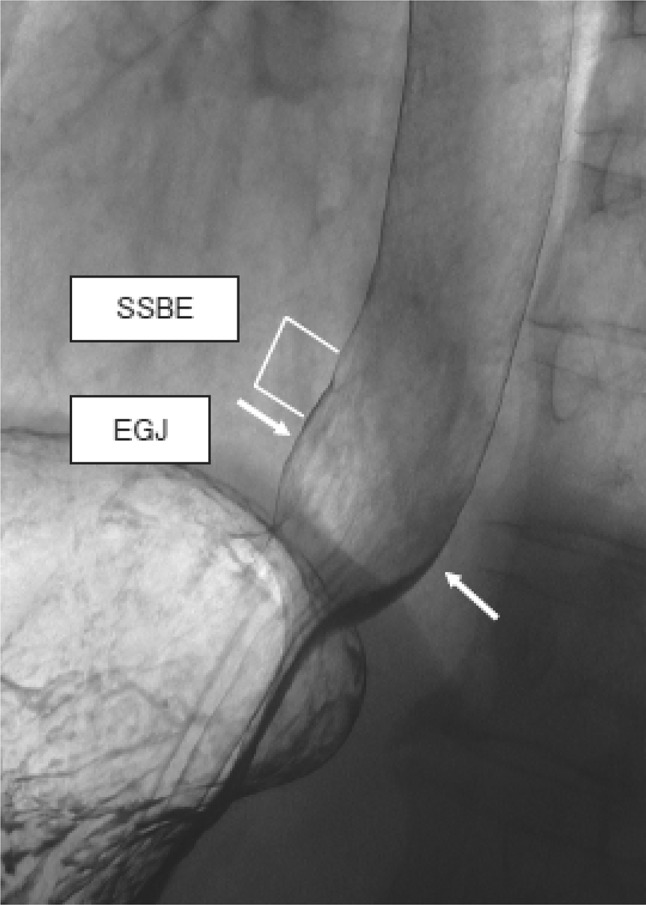
Barium contrast image of the EGJ in a subject with Barrett mucosa
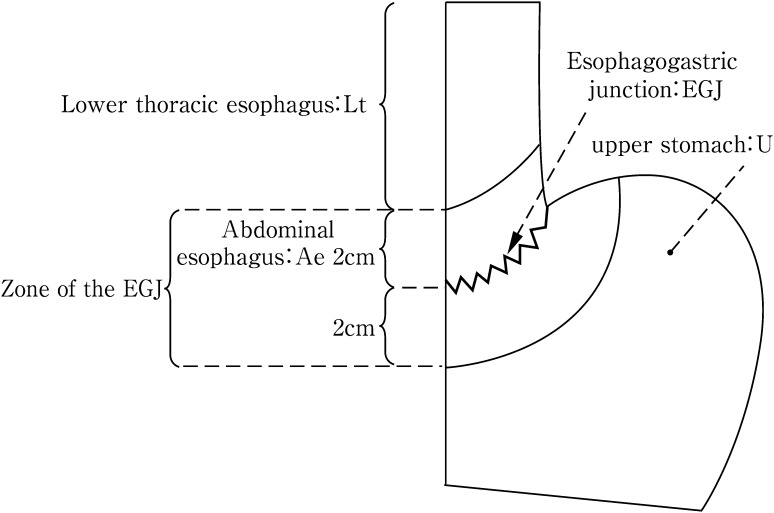
Definition and description of esophagogastric junction according to Nishi’s classification
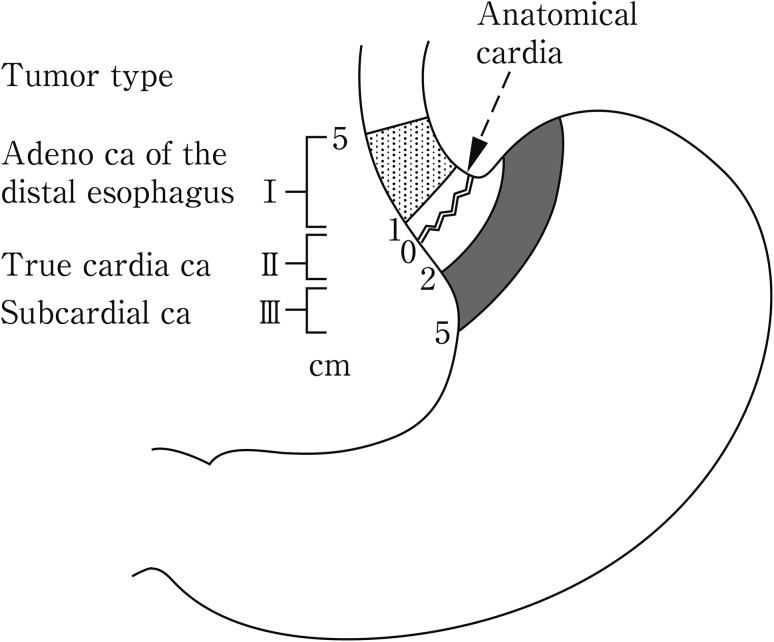
Definition and description of adenocarcinoma at the esophagogastric junction according to Siewert’s classification
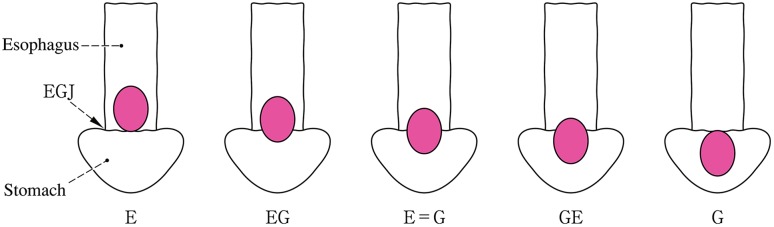
Subclassification and methods of description of cancer at the esophagogastric junction
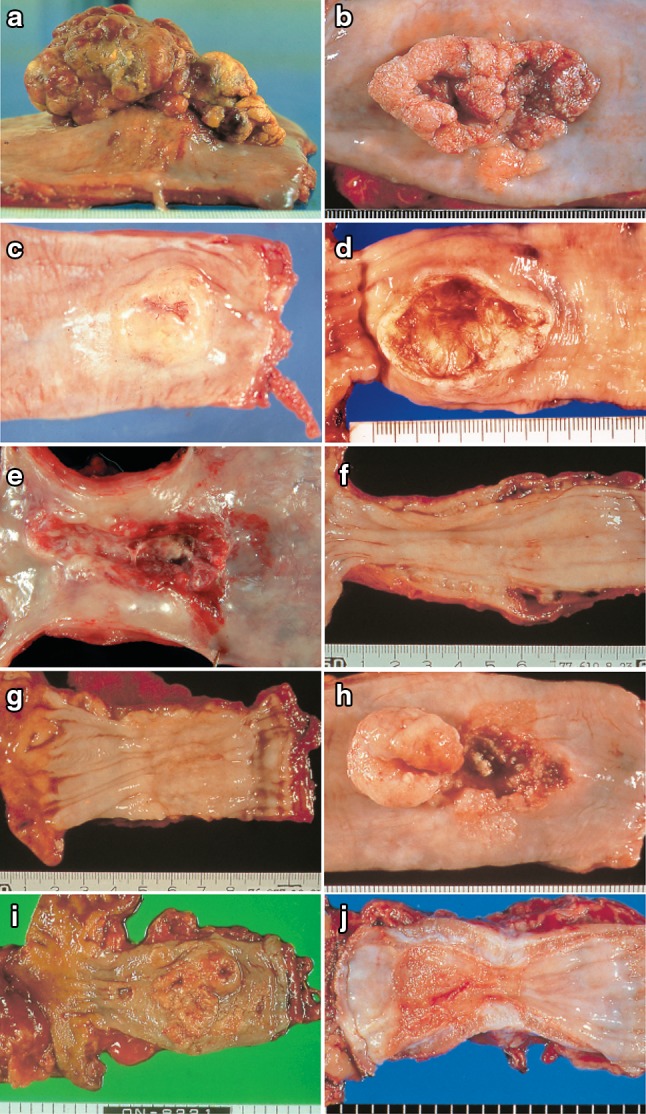
a Type 1: a pedunculated and tall polypoid lesion. This was judged to be advanced cancer based on its size, mobility (or cut cross section). b Type 1: this protruding type lesion with a clearly demarcated border has lobules or a papillary appearance on its surface. c Type 1: most of the surface of the protrusion is covered by non-cancerous epithelium. This was judged to be advanced cancer based on its size and immobility. d Type 2: this lesion is a deep ulcer with a well-demarcated surrounding ridge. Macroscopic findings: advanced type (Types 1–5). e Type 3: this lesion is a deep ulcer surrounded by a poorly demarcated ridge. The lesion extended circumferentially causing luminal stenosis. f Type 4: this diffusely invasive lesion with no clear margin makes the esophageal wall thick and hard, and causes luminal stenosis. No distinct ulcer can be seen. g Type 4: the thickening of the esophageal wall and the edematous changes of the mucosa suggest diffuse intramural extension of the lesion, but there is no finding of hardening or stenosis, and no finding of ulcer formation. h Combined type: this cancer showed mixed morphology of advanced Type 1 and Type 2 (0-IIc Type extension can be seen in part). i Type 5a: the macroscopic appearance is extremely complex with Type 1, and Type 2 and others, and it is difficult to categorize. j Type 5b: this macroscopic tumor (Type 5b) cannot be categorized because of preoperative chemoradiotherapy. i Type 5a: the macroscopic appearance is extremely complex with Type 1, and Type 2 and others, and it is difficult to categorize. j Type 5b: This macroscopic tumor (Type 5b) cannot be categorized because of preoperative chemoradiotherapy

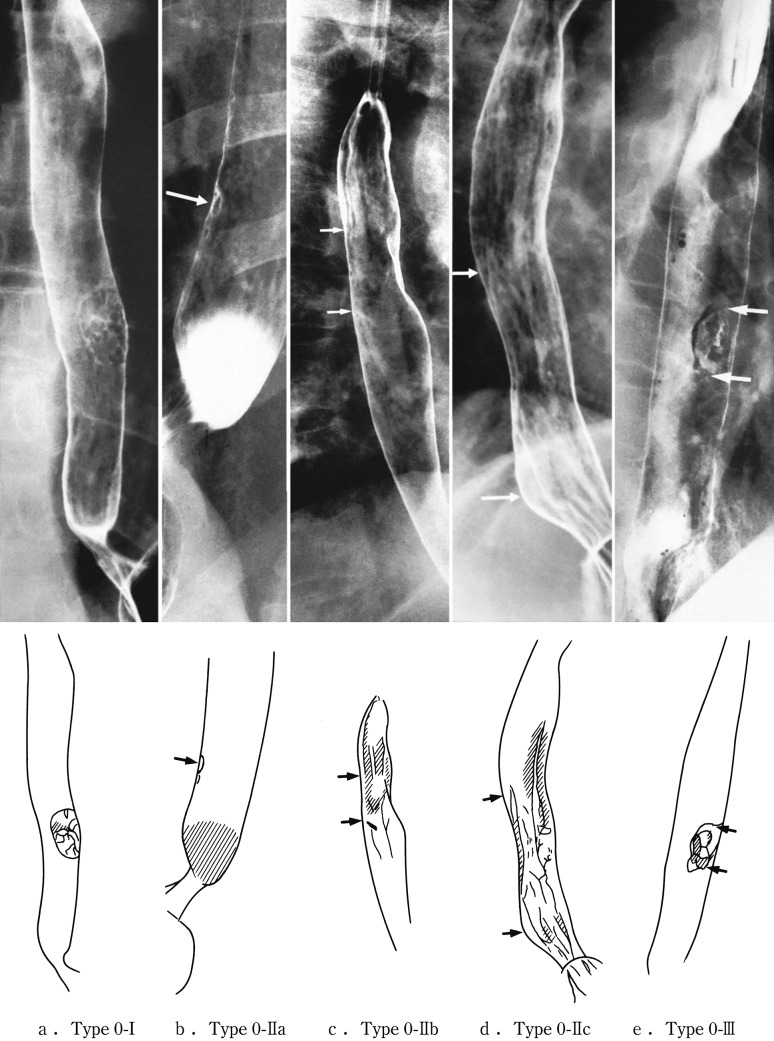
Roentgenological findings: advanced type
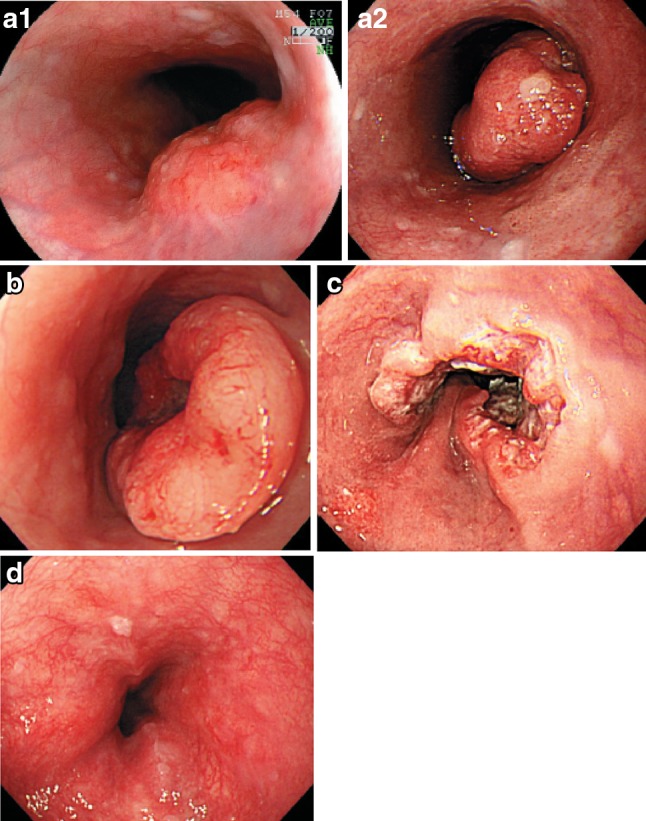
Endoscopic findings: advanced type. a1 Type 1, protruding type (pT2): a tall lesion with a broad base. a2 Type 1, protruding type (pT2): a tall lesion with a narrow base. b Type 2, ulcerative and localized type (pT3): a deep ulcerative lesion surrounded by a well-demarcated ridge. c Type 3, ulcerative and infiltrative type (pT3): a deep ulcerative lesion surrounded by an ill-demarcated ridge. d Type 4, diffusely infiltrative type (pT3): ill-defined thickening and hardening of the esophageal wall accompanied by luminal stenosis is observed. There is no remarkable ulcer formation
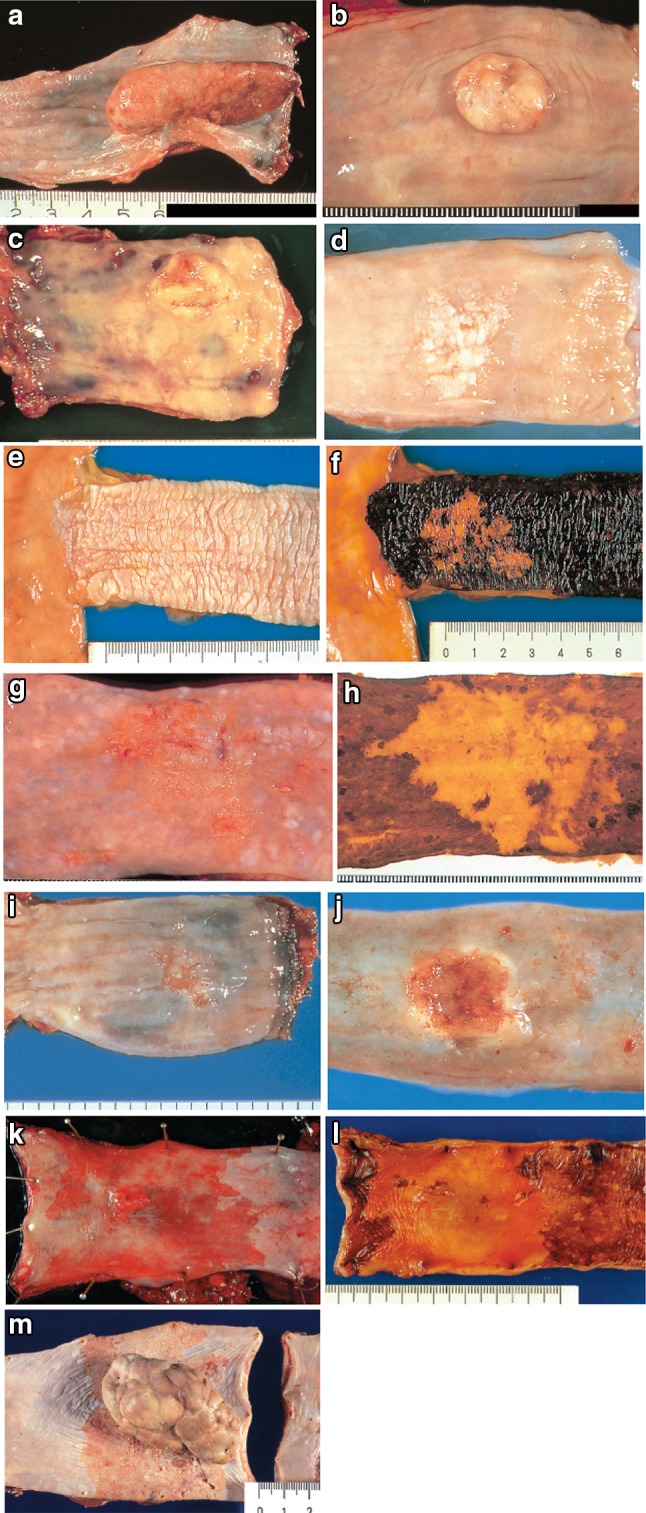
Macroscopic findings: superficial type (0 type). a Type 0-Ip (superficial and protruding type, pedunculated): The tumor is well demarcated and has a narrow base. b Type 0-Ip (superficial and protruding type, pedunculated): The well-demarcated, protruding tumor has an irregular and nodular surface. c Type 0-Is (superficial and protruding type, sessile): the surface of this ill-demarcated tumor is mostly covered by the normal epithelium. d Type 0-IIa (slightly elevated type): the tumor is only slightly elevated from the mucosa. Its color is generally white. e Type 0-IIb (flat type): there are only minute irregularities and no macroscopic abnormal features. f Type 0-IIb (flat type) (iodine-stained view of e) the superficial tumor can now be seen unstained by iodine. g Type IIc (slightly depressed type): the superficial depressed lesion has no clear margin and a finely granular surface. h (iodine-stained view of g): the superficial tumor is unstained by iodine. i Type 0-IIc (slightly depressed type): the superficial depressed lesion has an irregular margin. j Type 0-III (superficial and depressed type): the deeply depressed lesion with a slightly elevated margin suggests invasion beyond the muscularis mucosae. k Type 0-IIc+”0-IIa” (superficial spreading type): the widespread slightly depressed red lesion (0-IIc) has a slightly elevated lesion (0-IIa) in its center, suggesting invasion into the submucosal layer. The lesion, more than 5 cm in length, is defined as the superficial spreading type. l Type 0-IIc+”0-IIa” (superficial spreading type) (iodine-stained view of k): the reddish depressed lesion is not stained with iodine solution. m Type 0-IIc + “0-Ip”: the well-demarcated protruding tumor with a narrow base (0-Ip) has a slightly depressed lesion (0-IIc) in the surrounding area. This macroscopic appearance is characterized as carcinosarcoma
Radiological findings: superficial type
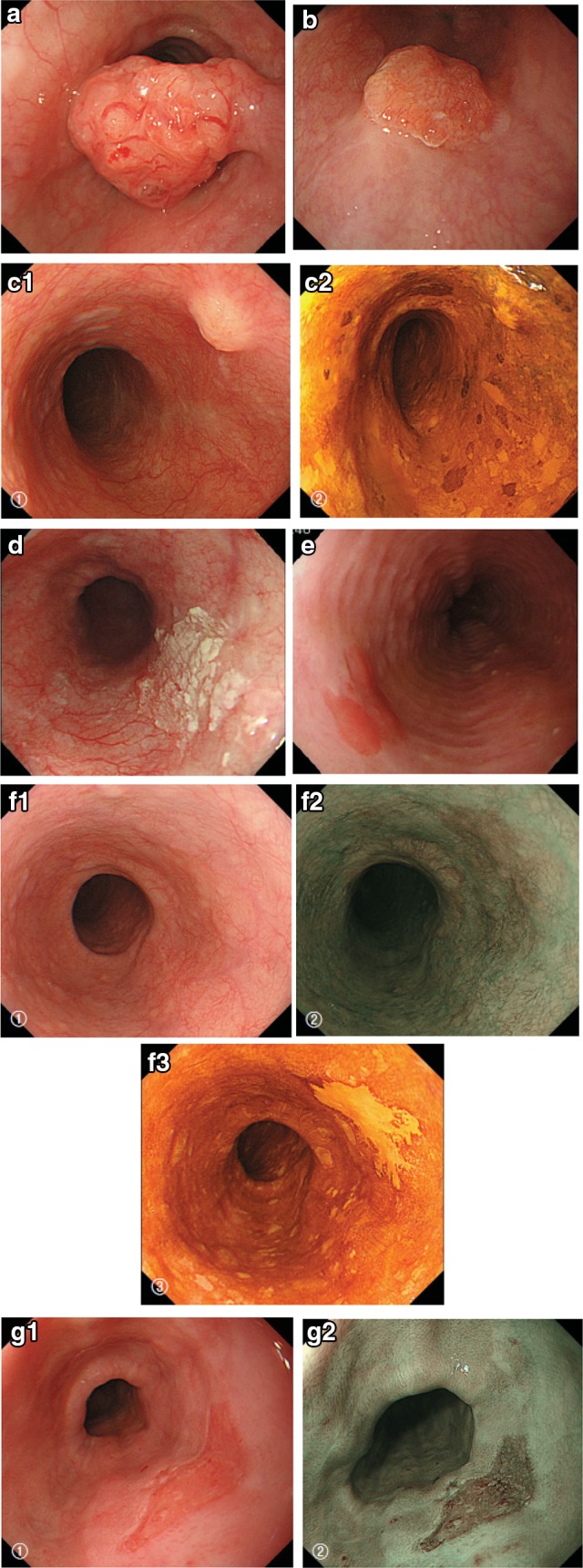
Endoscopic findings: superficial type. a Type 0-Ip, superficial and protruding type, pedunculated (cT1b-SM2-3): a well-demarcated protruding and pedunculated tumor shows an irregular and nodular surface. b Type 0-Is, superficial and protruding type, sessile (pT1b-SM2): a well-demarcated protruding and sessile tumor. c Type 0-Is, superficial and protruding type, sessile (pT1b-SM2): ➀ Conventional endoscopy: an ill-demarcated protruding tumor covered by normal esophageal mucosa suggests a tumor mass in the submucosa. ➁ Iodine staining: the mucosa covering the tumor is stained brown, and an unstained area at the top suggests exposed tumor tissue. d Type 0-IIa, slightly elevated type (pT1a-MM): a plaque-like, slightly elevated white tumor. Tumor invasion of the white area remained within the lamina propria, while a tiny protrusion at the distal margin of the tumor had invaded the muscularis mucosae. e Type 0-IIa, slightly elevated type (pT1a-EP): a slightly elevated tumor with well-demarcated reddening (the height of a type 0-IIa lesion is less than 1 mm). f Type 0-IIb flat type (pT1a-EP): ➀ Conventional endoscopy: a conventional observation could not detect the lesion. ➁ Narrow band imaging shows a brownish area. ➂ Iodine staining: a completely flat lesion was identified as a well-demarcated, unstained area using iodine staining. g Type 0-IIc, slightly depressed type (pT1a-LPM). ➀ Conventional endoscopy: an irregularly shaped mucosal reddening with a slight depression is visible. ➁ Narrow band imaging: the lesion is also visible as a brownish area. ➂ Iodine staining: a well-demarcated, unstained area is visible using iodine staining. h Type 0-IIc, slightly depressed type (pT1b-SM1): ➀ Conventional endoscopy: an area of mucosal reddening with a slight depression and marginal elevation is visible. ➁ Narrow band imaging: a brownish area suggesting a hypervascular lesion is visible. i Type 0-III, superficial and excavated type (cT1b-SM2-3). ➀ Conventional endoscopy, ➁ narrow band imaging (cT1b-SM2-3): a distinctly depressed lesion with a surrounding elevated area is visible using conventional observations, suggesting an ulcer reaching the muscularis mucosa. j Combined type 0-IIc + “0-Is” (pT1b-SM2): ➀ Conventional endoscopy: a distinct elevation with a wide base is visible. A slightly depressed lesion was also noted close to the distal margin of the lesion. ➁ Narrow band imaging: a lesion with a well-demarcated margin is visible. k Combined type 0-Is + 0-IIc (pT1b-SM2): ➀ Conventional endoscopy: a distinctly protruding lesion with a wide base and irregular, nodular changes is visible. Reddening of the esophageal mucosa close to the lesion with an ill-defined margin was suspected. ➁ Iodine staining: The margins of the mucosal changes were identified as well-demarcated, unstained areas
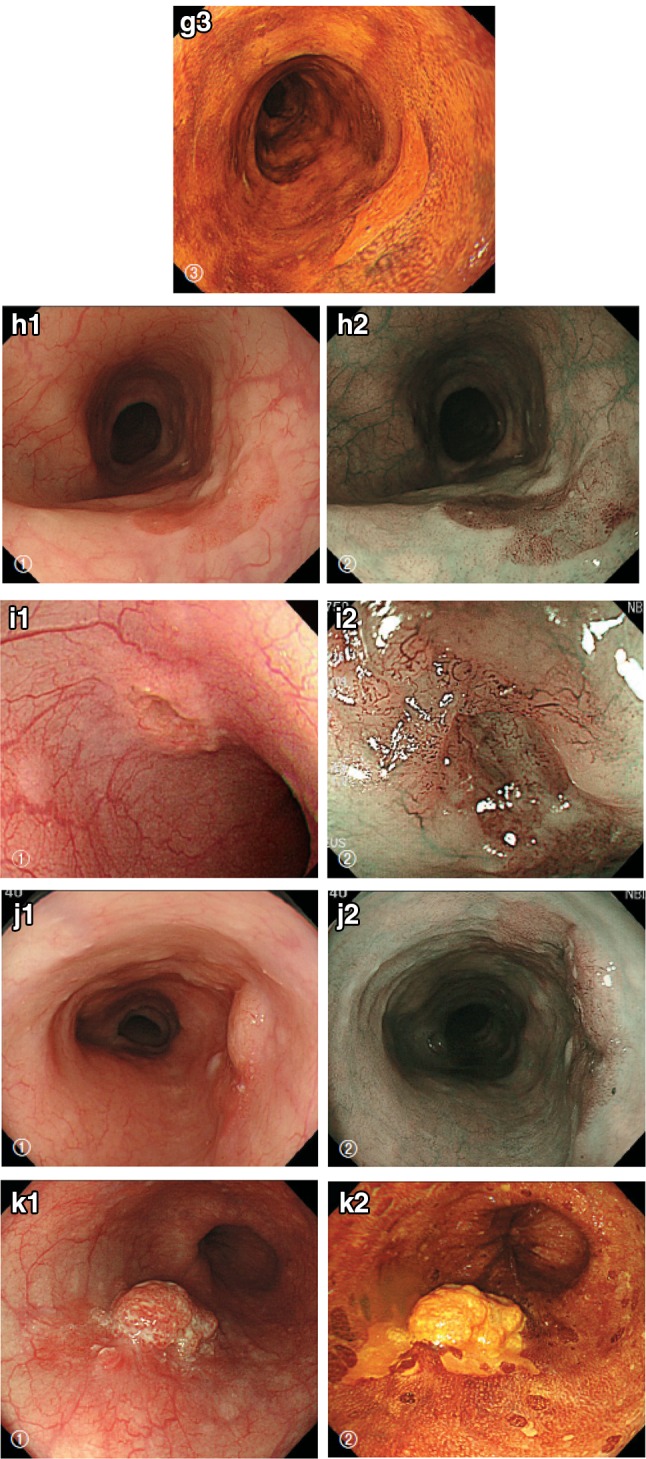
Endoscopic findings: superficial type. a Type 0-Ip, superficial and protruding type, pedunculated (cT1b-SM2-3): a well-demarcated protruding and pedunculated tumor shows an irregular and nodular surface. b Type 0-Is, superficial and protruding type, sessile (pT1b-SM2): a well-demarcated protruding and sessile tumor. c Type 0-Is, superficial and protruding type, sessile (pT1b-SM2): ➀ Conventional endoscopy: an ill-demarcated protruding tumor covered by normal esophageal mucosa suggests a tumor mass in the submucosa. ➁ Iodine staining: the mucosa covering the tumor is stained brown, and an unstained area at the top suggests exposed tumor tissue. d Type 0-IIa, slightly elevated type (pT1a-MM): a plaque-like, slightly elevated white tumor. Tumor invasion of the white area remained within the lamina propria, while a tiny protrusion at the distal margin of the tumor had invaded the muscularis mucosae. e Type 0-IIa, slightly elevated type (pT1a-EP): a slightly elevated tumor with well-demarcated reddening (the height of a type 0-IIa lesion is less than 1 mm). f Type 0-IIb flat type (pT1a-EP): ➀ Conventional endoscopy: a conventional observation could not detect the lesion. ➁ Narrow band imaging shows a brownish area. ➂ Iodine staining: a completely flat lesion was identified as a well-demarcated, unstained area using iodine staining. g Type 0-IIc, slightly depressed type (pT1a-LPM). ➀ Conventional endoscopy: an irregularly shaped mucosal reddening with a slight depression is visible. ➁ Narrow band imaging: the lesion is also visible as a brownish area. ➂ Iodine staining: a well-demarcated, unstained area is visible using iodine staining. h Type 0-IIc, slightly depressed type (pT1b-SM1): ➀ Conventional endoscopy: an area of mucosal reddening with a slight depression and marginal elevation is visible. ➁ Narrow band imaging: a brownish area suggesting a hypervascular lesion is visible. i Type 0-III, superficial and excavated type (cT1b-SM2-3). ➀ Conventional endoscopy, ➁ narrow band imaging (cT1b-SM2-3): a distinctly depressed lesion with a surrounding elevated area is visible using conventional observations, suggesting an ulcer reaching the muscularis mucosa. j Combined type 0-IIc + “0-Is” (pT1b-SM2): ➀ Conventional endoscopy: a distinct elevation with a wide base is visible. A slightly depressed lesion was also noted close to the distal margin of the lesion. ➁ Narrow band imaging: a lesion with a well-demarcated margin is visible. k Combined type 0-Is + 0-IIc (pT1b-SM2): ➀ Conventional endoscopy: a distinctly protruding lesion with a wide base and irregular, nodular changes is visible. Reddening of the esophageal mucosa close to the lesion with an ill-defined margin was suspected. ➁ Iodine staining: The margins of the mucosal changes were identified as well-demarcated, unstained areas
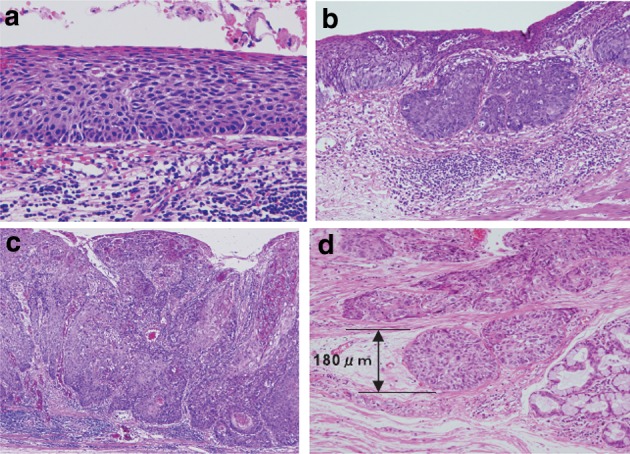
Diagnostic criteria for depth of invasion. a T1a-EP (Tis): carcinoma in situ. b T1a-LPM: tumor has invaded the lamina propria mucosae. c T1a-MM: tumor has invaded the muscularis mucosae. d T1b-SM1: tumor invasion is limited to the upper third of the submucosal layer. The vertical depth of invasion is 180 μm from the lower edge of the muscularis mucosae. The lesion was diagnosed as pT1b-SM1 in the endoscopically resected specimen
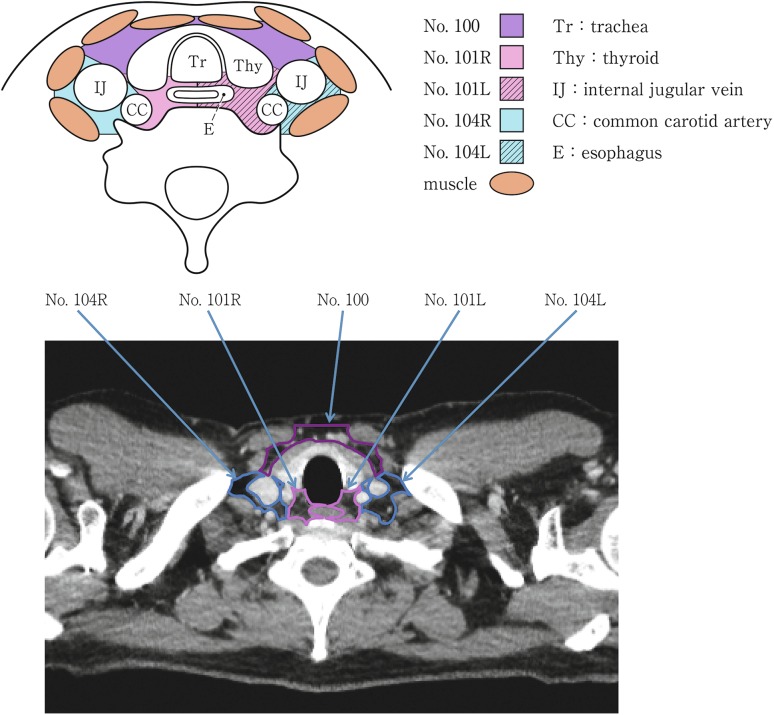
Cervical lymph nodes. Tr tracheal, Thy thyroid, IJ internal jugular vein, CC common carotid artery, E esophagus
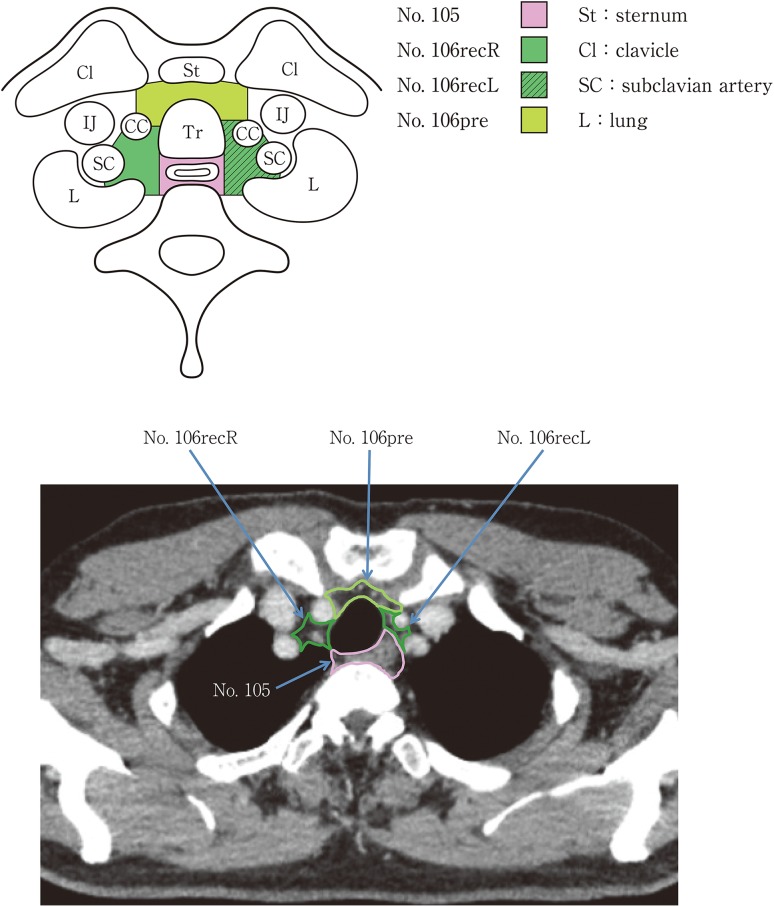
Superior mediastinal lymph nodes
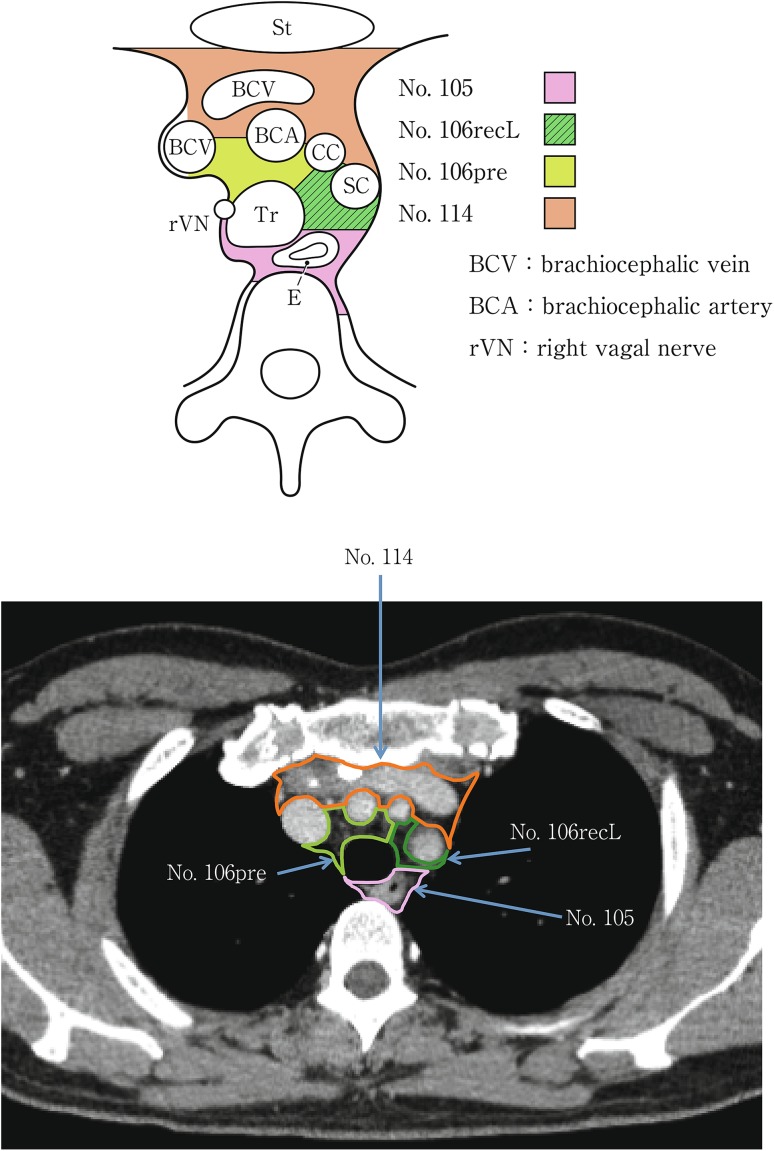
Upper mediastinal lymph nodes in the level above the aortic arch
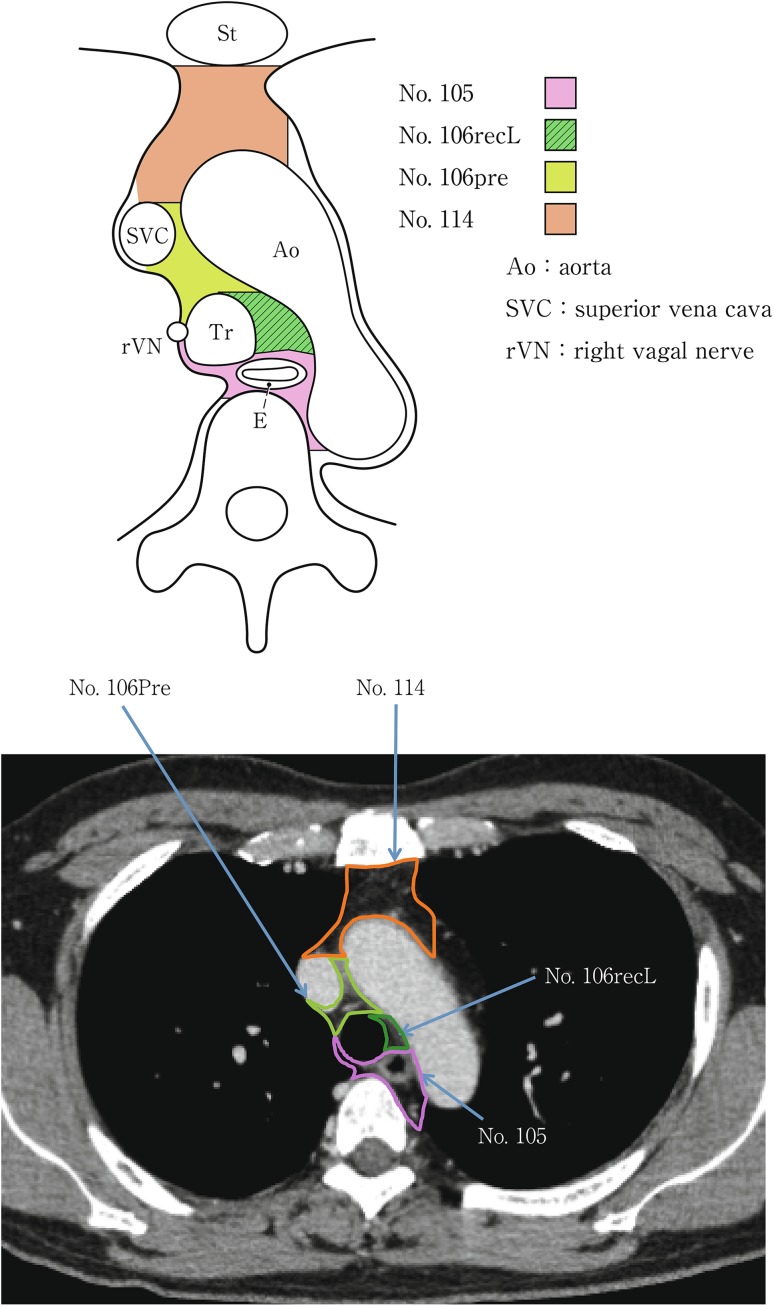
Upper mediastinal lymph nodes at the level of the aortic arch
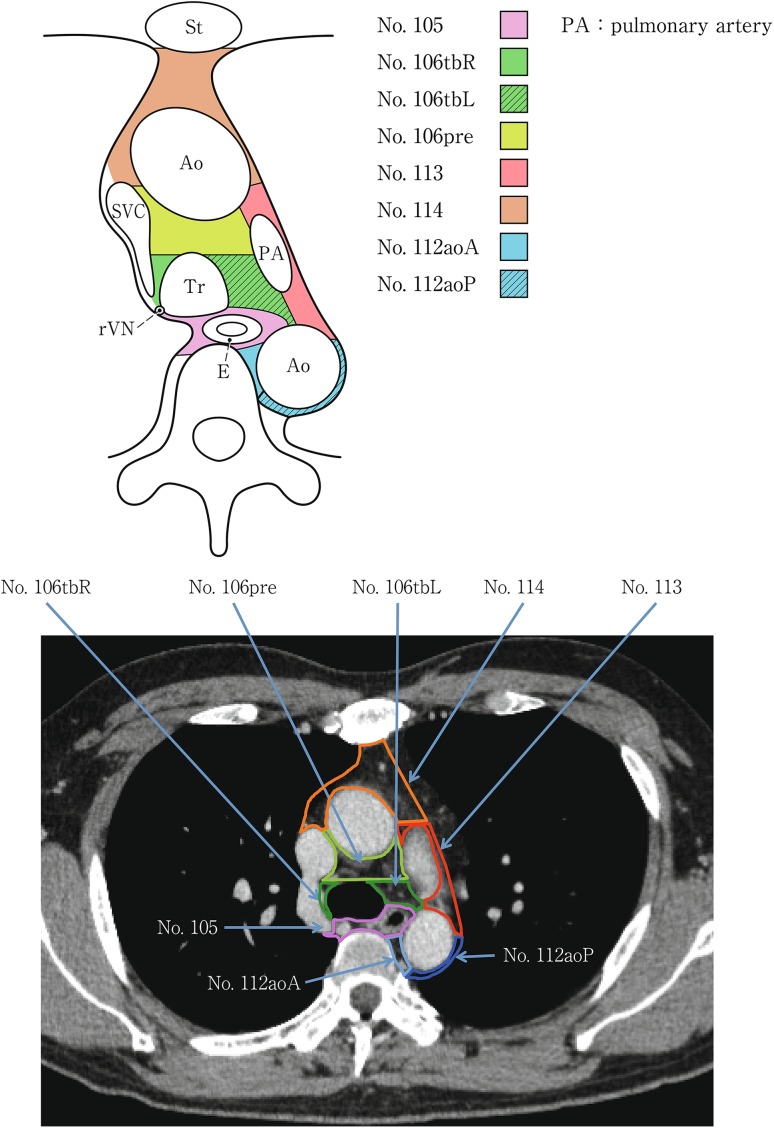
Upper mediastinal lymph nodes in the level below the aortic arch
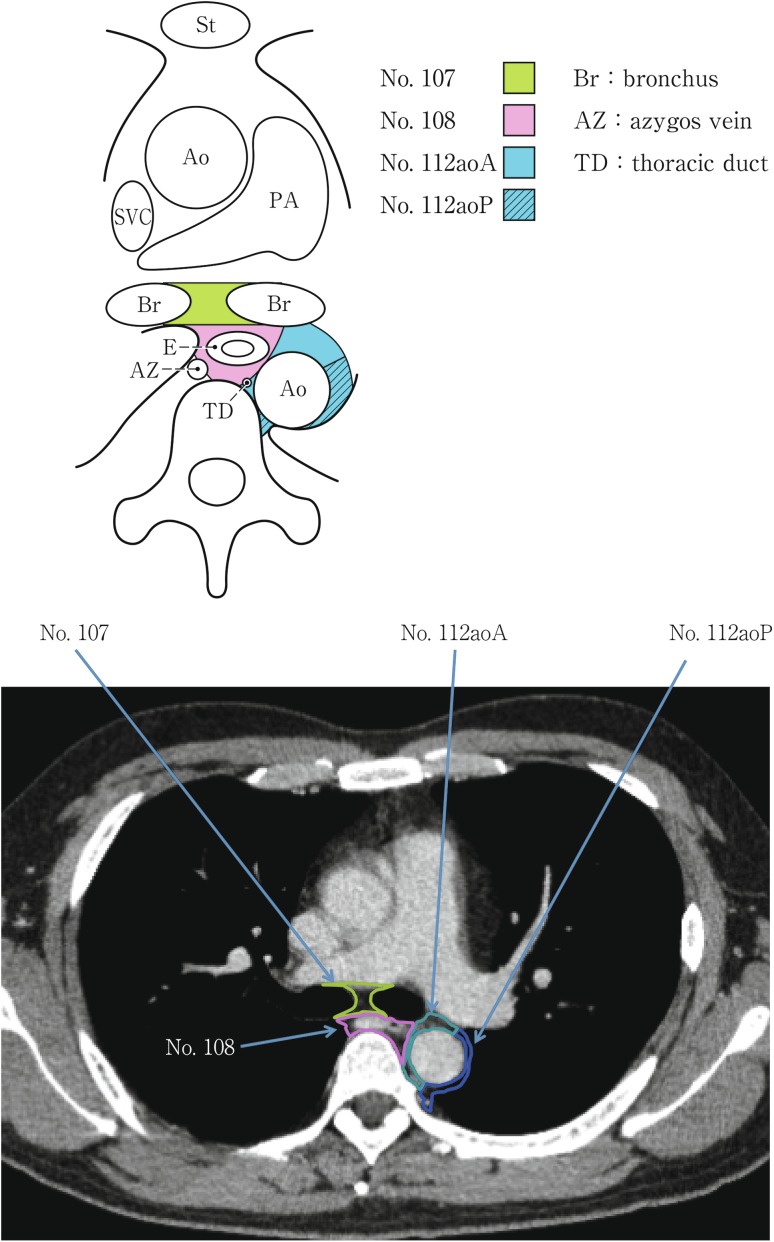
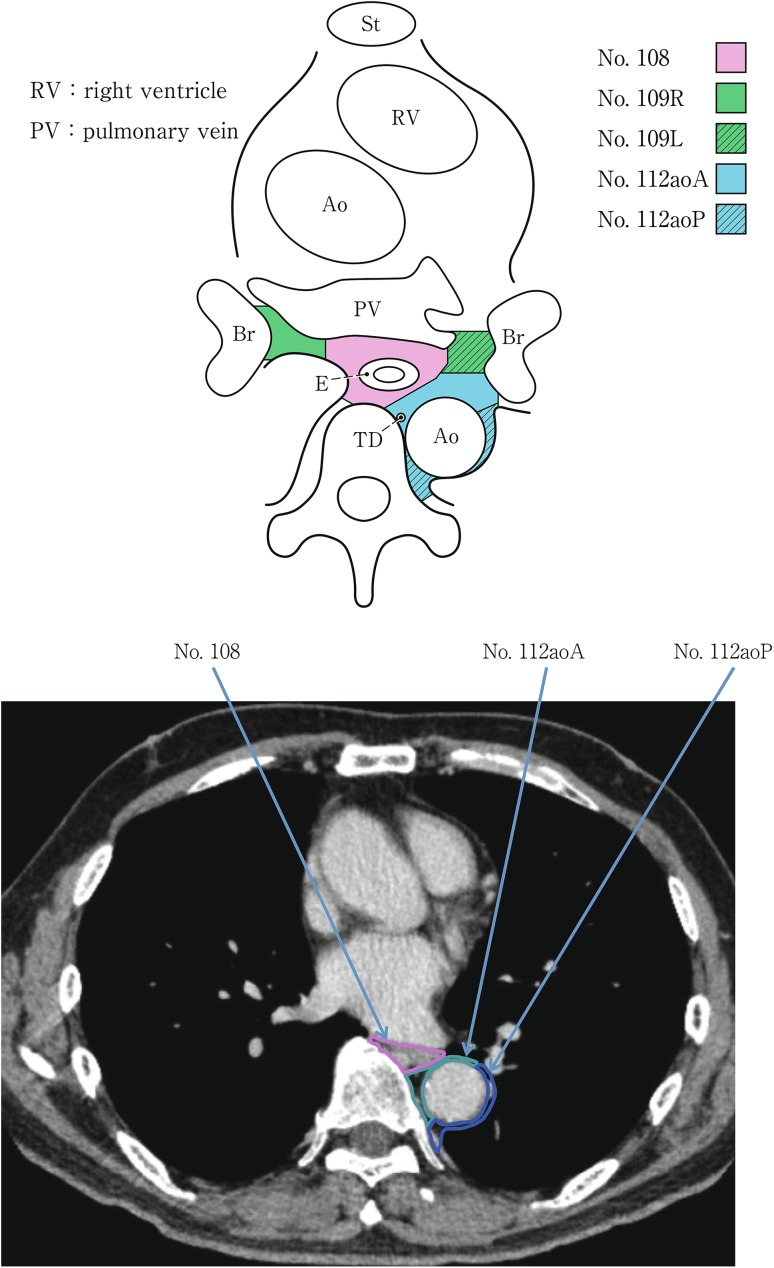
Mediastinal lymph nodes in the level below the carina
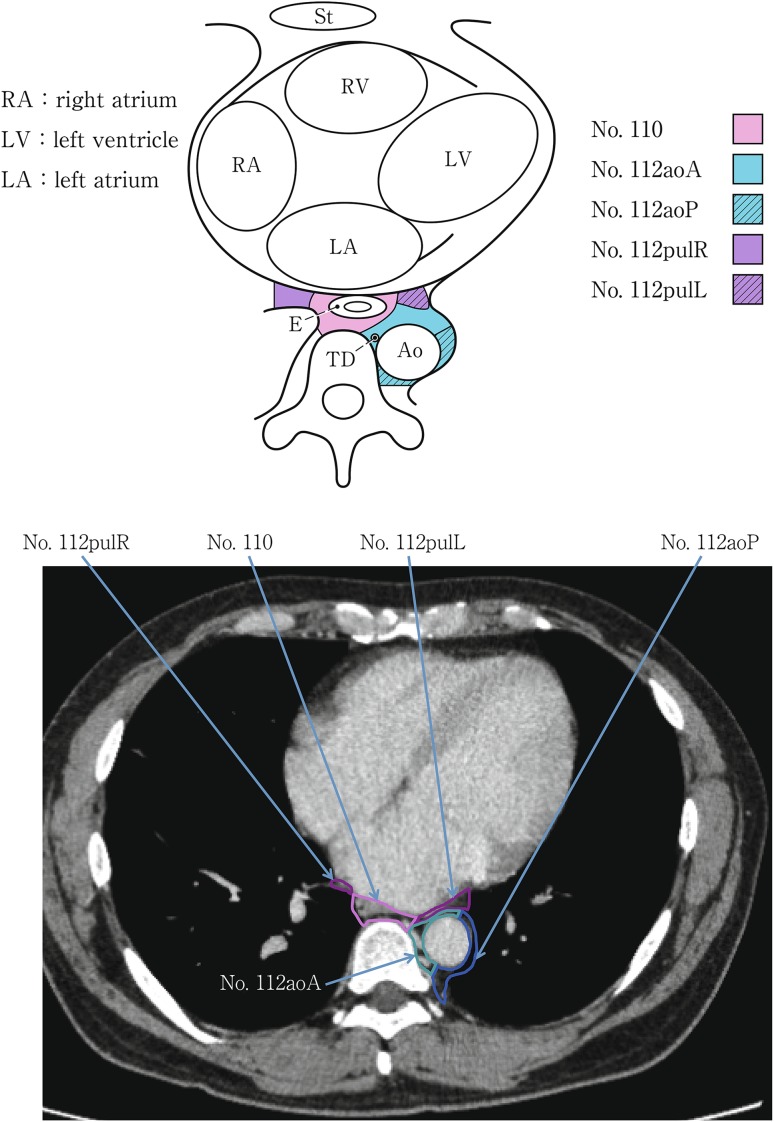
Lower mediastinal lymph nodes in the level of the inferior pulmonary vein
Lower mediastinal lymph nodes in the level of the right atrium
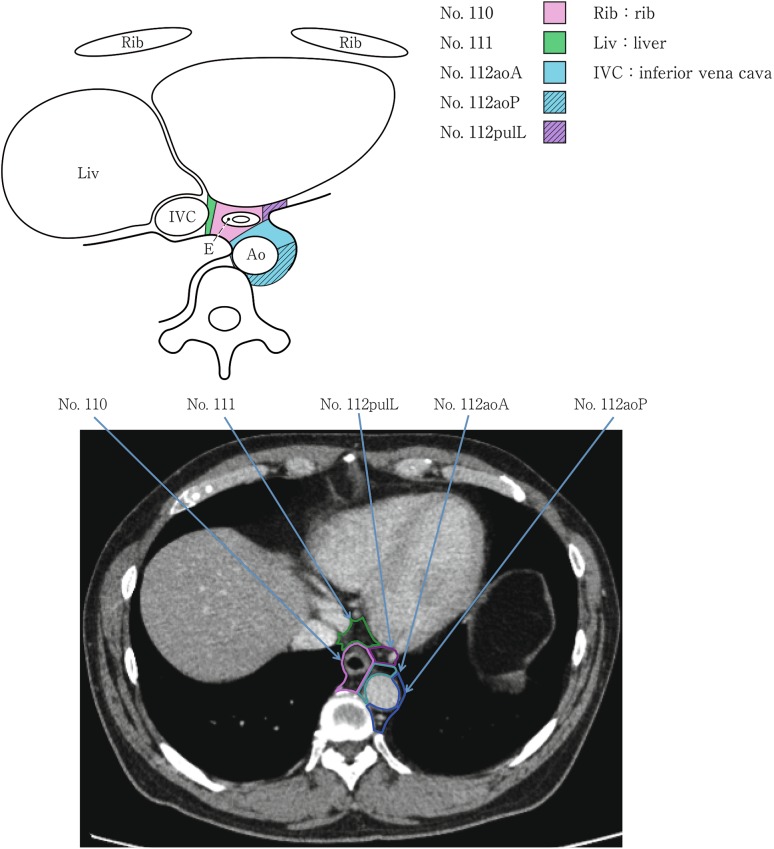
Lower mediastinal lymph nodes in the level above the hiatus
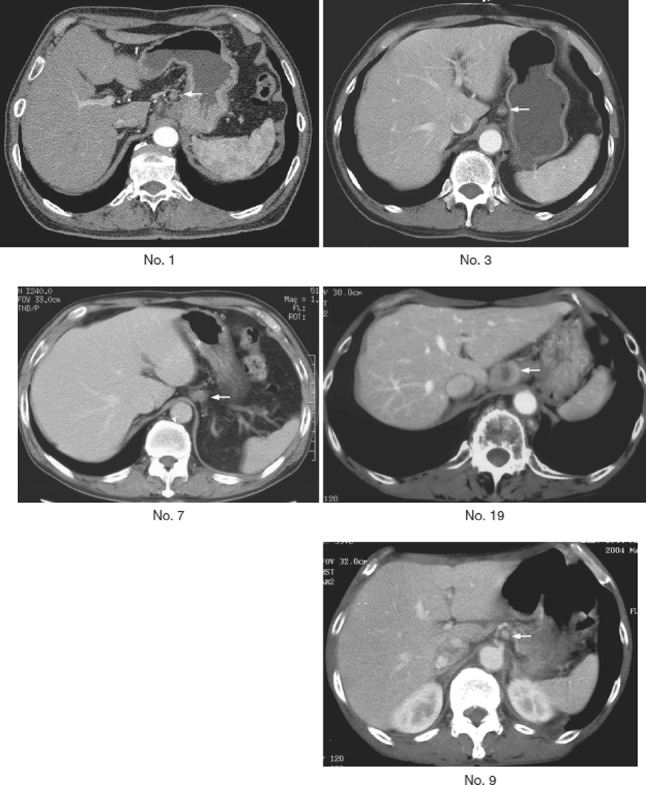
Abdominal lymph nodes
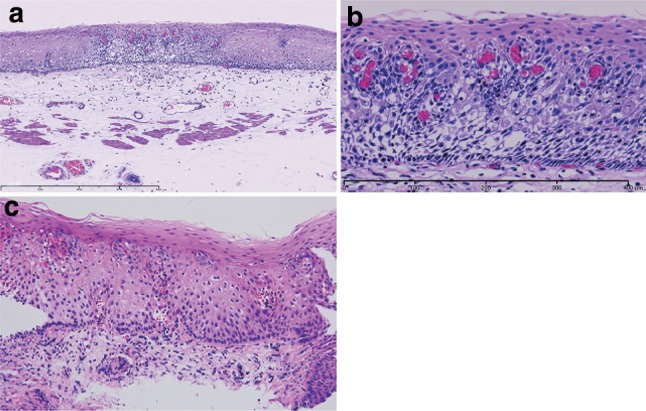
Squamous intraepithelial neoplasia. a Low magnification of squamous intraepithelial neoplasia. The lesion is visible as an iodine-unstained area measuring 3 mm in size. Histologically, the lesion is well demarcated. b High magnification. The tumor shows mild nuclear atypia with low cellular density and a regular arrangement of the basal layer. c Histology of biopsy specimen. The lesion is visible as an iodine-stained tan area measuring 5 mm in size. Histopathologically, a mildly thickened epithelium exhibits atypical cell proliferation in the lower two-thirds of the epithelium, but nuclear atypia is mild and the basal layer has a regular arrangement
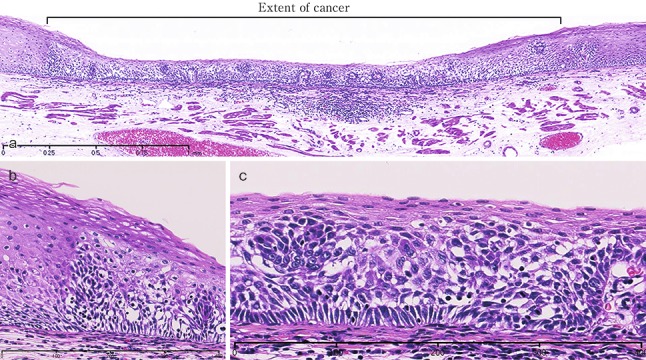
Squamous cell carcinoma (pT1a-EP). a Low-power view of squamous cell carcinoma. The border between the carcinoma and non-neoplastic epithelium is clear. b Histology of the border between the squamous cell carcinoma and the non-neoplastic squamous epithelium. The cancer tissue exhibits a high cellular density with a loss of the basal layer. c Histology of the central portion of cancer tissue. The cancer cells have proliferated throughout the entire epithelial layer, but have not invaded the lamina propria mucosae
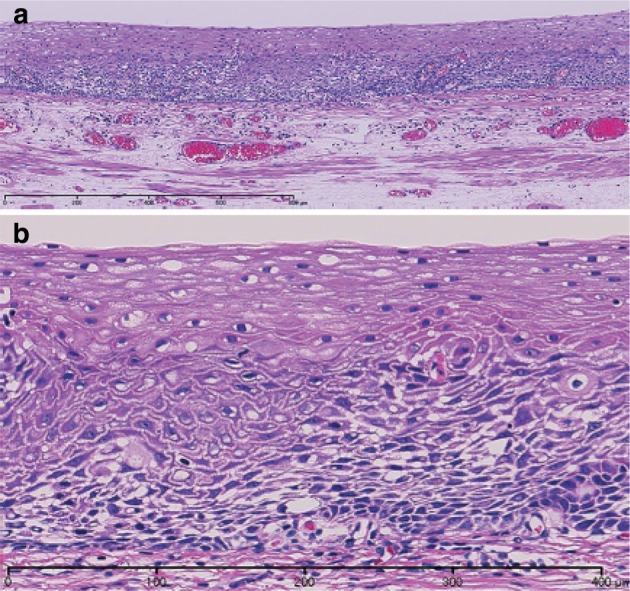
Basal layer-type squamous cell carcinoma (pT1a-EP). a Cancer cells are present within the lower half of the epithelium, whereas squamous epithelial cells with minimal atypia are present in the upper half. b High-power view of the above figure. The basal cells have disappeared and the lower half of the epithelium has been replaced by cancer cells with nuclear atypia and a higher cellular density. Squamous epithelial cells in the upper half are small in size and have a lower cellular density
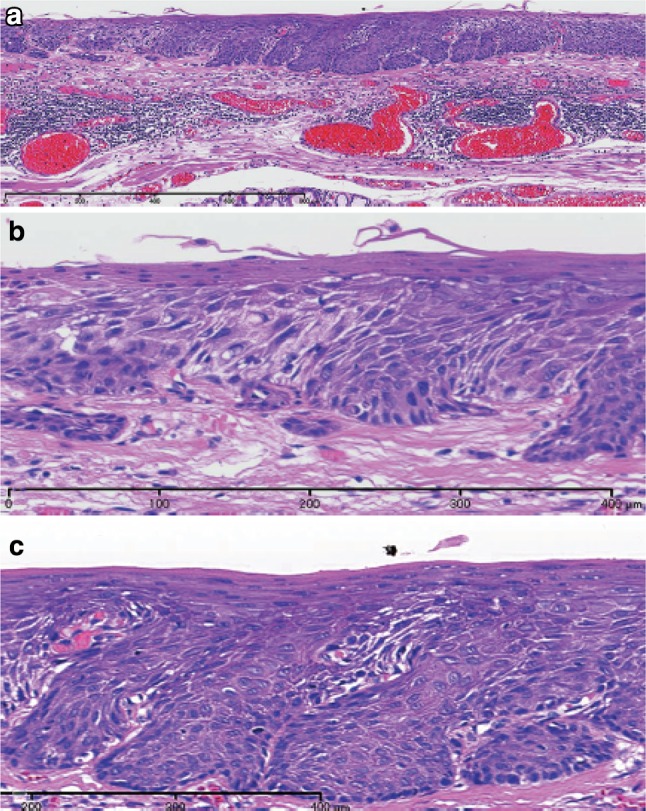
Squamous cell carcinoma with invasion into the lamina propria mucosae (pT1a-LPM). a Squamous cell carcinoma shows mild thickening and irregular downward growth. b Droplet infiltration is observed in the lamina propria mucosae. c Expansive growth of squamous cell carcinoma
Squamous cell carcinoma with invasion into the muscularis mucosae (pT1a-MM). a Cancer cells have reached the upper end of the muscularis mucosae and have partly invaded the muscularis mucosae. Both situations are classified as pT1a-MM. b Cancer cells have invaded the muscularis mucosae, but not beyond
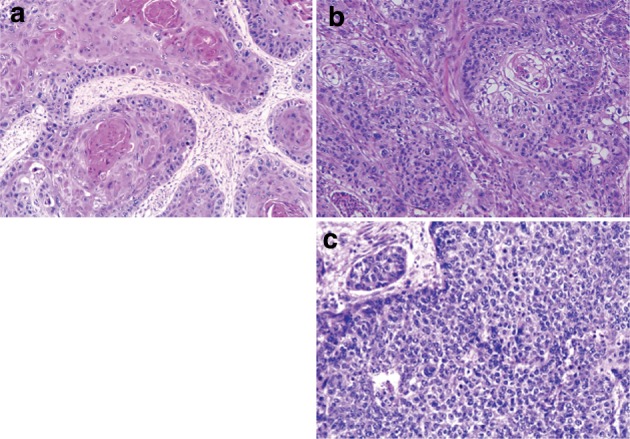
Squamous cell carcinoma. a Well differentiated squamous cell carcinoma: cancer pearls with marked keratinization are observed. b Moderately differentiated squamous cell carcinoma: sheet-like arrangement of tumor cells with slight keratinization is observed. c Poorly differentiated squamous cell carcinoma: keratinization is not observed, although tumor cells show sheet-like arrangement
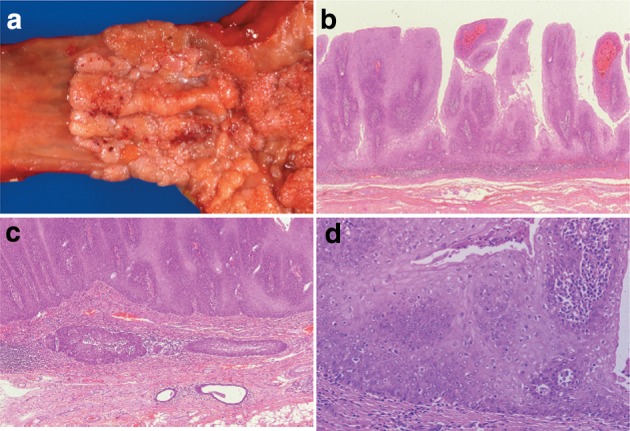
Verrucous squamous carcinoma. a Gross features of verrucous carcinoma. The tumor involves the cervical esophagus and lower pharynx. The tumor has a granular surface. b Low-power view of verrucous carcinoma. Note that papillary growth is prominent and the basal layer is generally flat. c Verrucous carcinoma with invasion into the lamina propria mucosae. d High-power view of verrucous carcinoma. The tumor has a high cellular density with an irregular arrangement at the basal site. However, squamous differentiation is apparent towards the surface
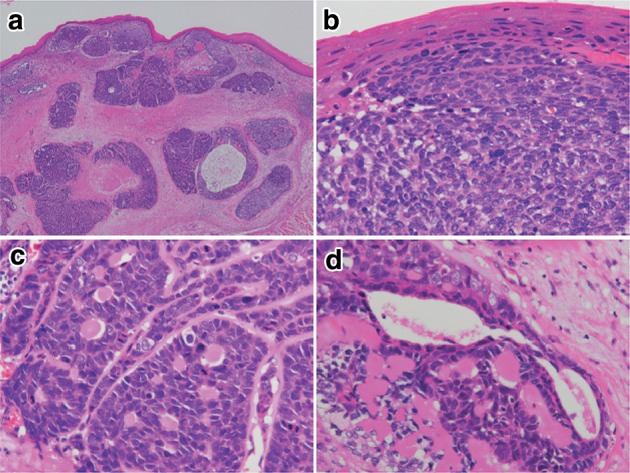
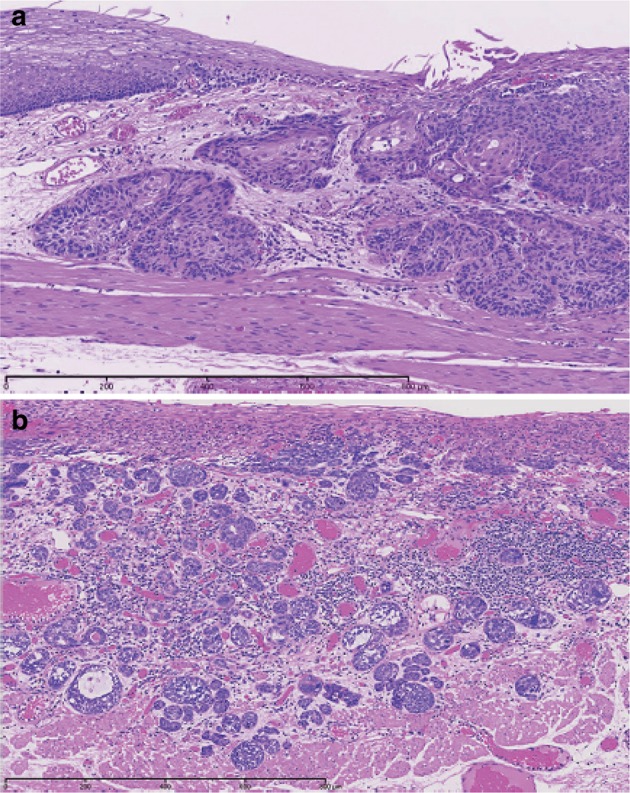
Basaloid squamous carcinoma. a Basaloid squamous carcinoma is often covered by non-neoplastic stratified squamous epithelium and grows downwards. The tumor forms a solid nest with occasional cyst formation and necrosis. b Tumor cells similar to basal cells form solid nests in various sizes under stratified squamous epithelium. c Tumor cells show a solid and trabecular arrangement. Eosinophilic basement membrane-like material deposits are present around and within the tumor nest. d Basaloid squamous carcinoma sometimes contains duct-like differentiation
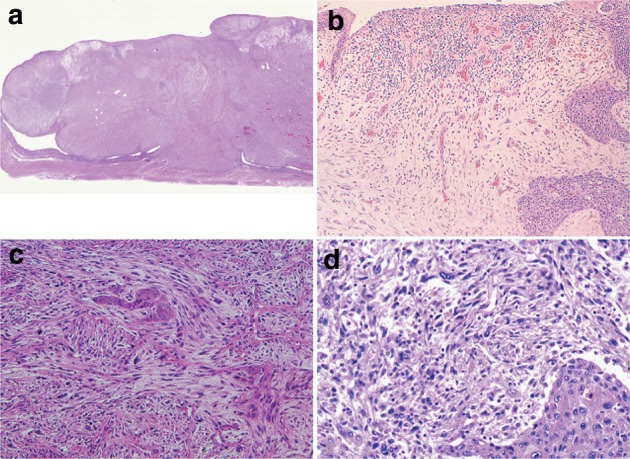
Carcinosarcoma. a A large tumor protrudes into the esophageal lumen. The tumor has not invaded deeply, in comparison with its size. b The polypoid tumor mainly consists of spindle cells, and its surface is covered by squamous cell carcinoma. c A large part of the tumor (sarcomatous component) is occupied by spindle-shaped tumor cells with scattered small foci of squamous cell carcinoma. d Tumor cells with prominent polymorphous nuclei are present in the sarcomatous component, which is similar to pleomorphic undifferentiated sarcoma (formerly diagnosed as malignant fibrous histiocytoma [MFH])
Adenocarcinoma in non-Barrett esophagus. a Well differentiated adenocarcinoma is observed proximal to the squamocolumnar junction. b Well differentiated adenocarcinoma is present beneath the squamous epithelium. Barrett mucosa is not observed, so that the origin of the tumor is unknown
Adenosquamous carcinoma. Adenosquamous carcinoma consists of squamous cell carcinoma and adenocarcinoma. Invasive squamous cell carcinoma is present on the oral side of the tumor, and adenocarcinoma is mainly present on the anal side
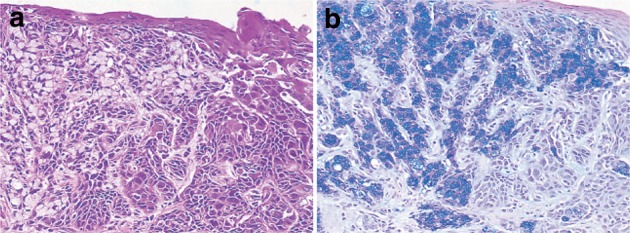
Mucoepidermoid carcinoma. a Signet ring cell carcinoma is observed within squamous cell carcinoma. b Mucus in signet ring cell carcinoma is stained blue by Alcian-blue staining. Serial section of a
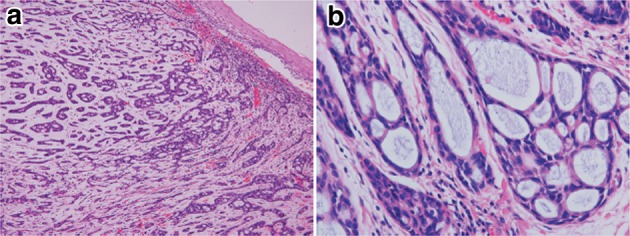
Adenoid cystic carcinoma. a A tumor with duct-like structures and a cribriform pattern has invaded downwards. b The histology of esophageal adenoid cystic carcinoma is almost the same as that with a salivary gland origin. Nuclear atypia is more prominent in the esophageal tumor than in the salivary gland tumor
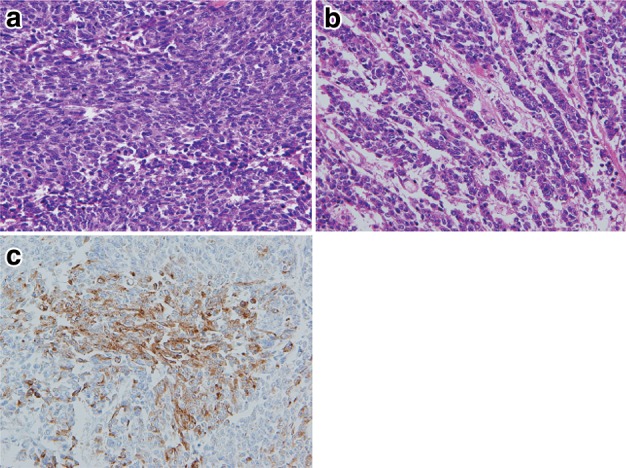
Neuroendocrine carcinoma, small cell type. a Small round cells with scant cytoplasm proliferate densely. b Tumor cells show an irregular arrangement with trabecular or ribbon-like patterns. c Immunohistochemically, the tumor cells are positive for chromogranin A, indicating differentiation to neuroendocrine cells
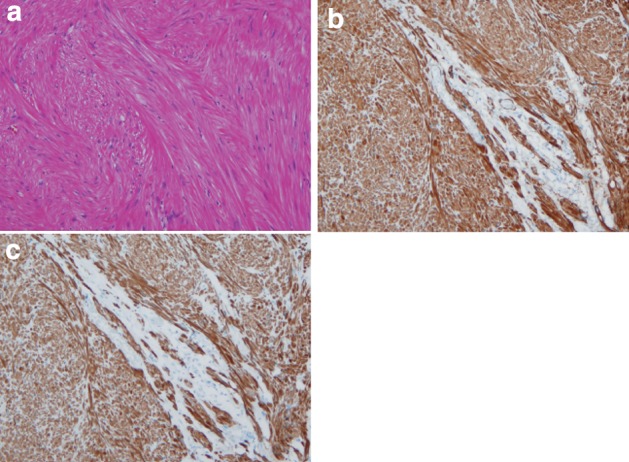
Leiomyoma. a Spindle cells with eosinophilic cytoplasm scantily grow in the fascicular pattern. b Immunohistochemically, the tumor cells are positive for α-smooth muscle actin. c Tumor cells are also positive for desmin
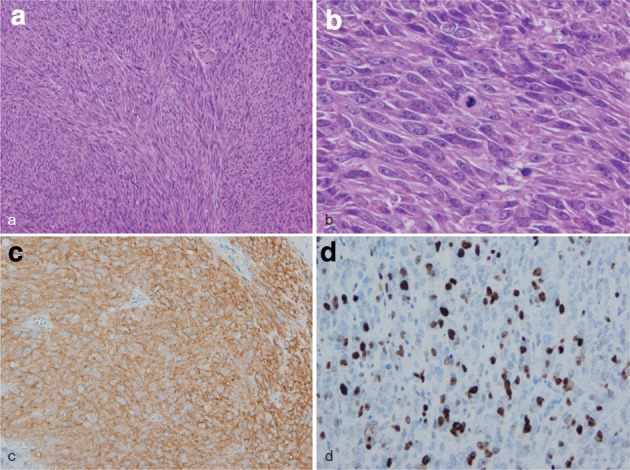
Gastrointestinal stromal tumor (GIST). a Spindle cells densely proliferate with fascicular arrangement. b Mitotic figures are shown among tumor cells with plump nuclei. c Immunohistochemically, the tumor cells are positive for KIT (CD117). d The Ki-67 (MIB-1) labeling index was 30%, indicating a high-risk tumor
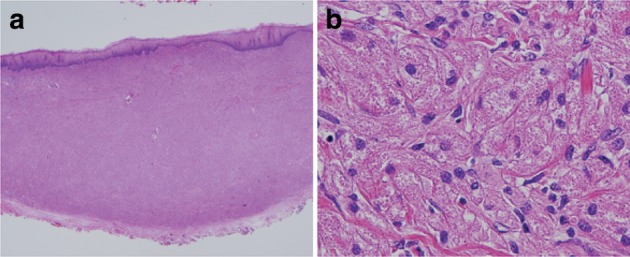
Granular cell tumor. a The tumor has grown mainly within the lamina propria mucosae and is covered by stratified squamous epithelium. b Large and round tumor cells exhibit abundant granular and eosinophilic cytoplasm
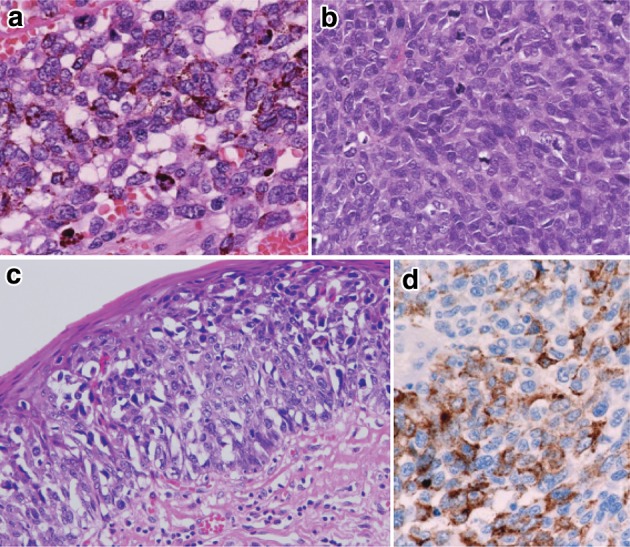
Malignant melanoma. a Short spindle-shaped or round tumor cells with abundant melanin granules have proliferated densely. b No melanin granules are observed in amelanotic melanoma. c Tumor cells with a clear cytoplasm show intraepithelial spread adjoining an invasive tumor. d Immunohistochemically, the tumor cells are positive for HMB-45 (Human Melanoma Black-45)
Resected specimen receiving chemoradiotherapy
Grade 1: slightly effective. a ×100. b ×200 high-magnification view of a
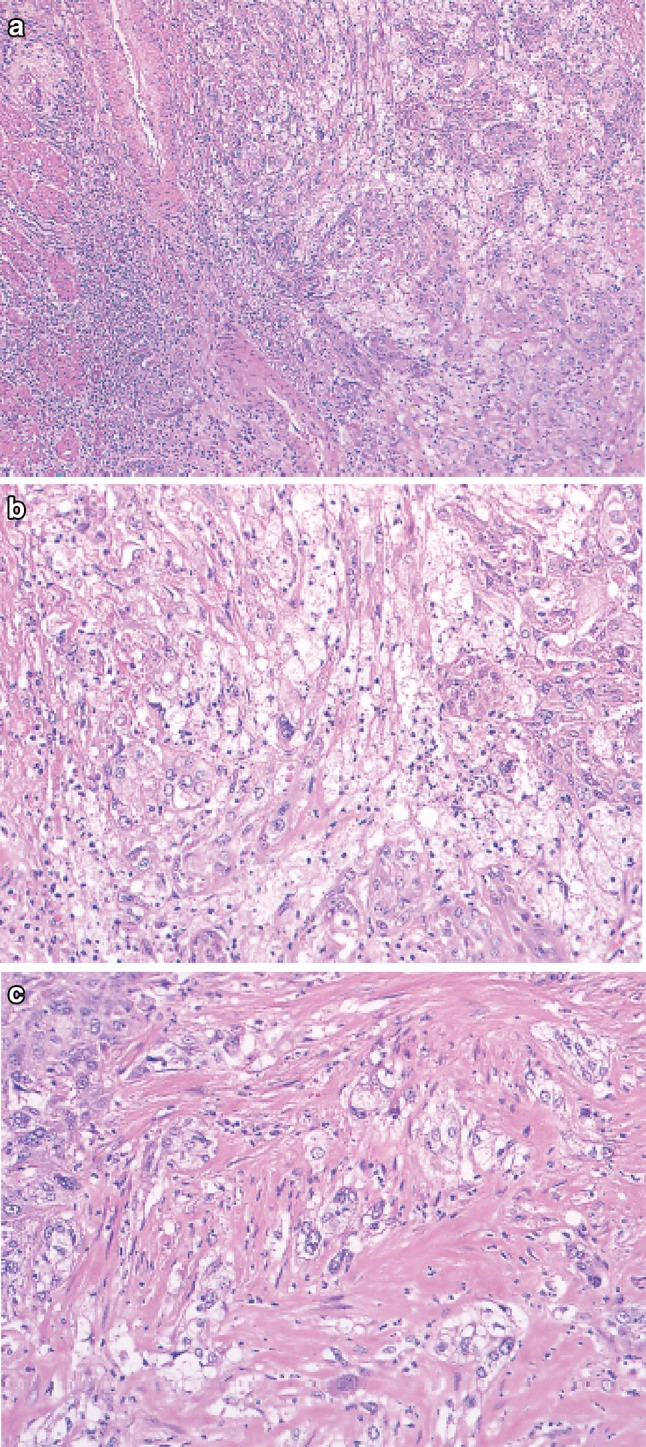
Grade 2: moderately effective. a ×100. b ×200 High-magnification view of a. a, b Small nests of a tumor are surrounded by macrophages with foamy cytoplasm. Most of the residual cancer cells show degeneration, and decreased staining with eosin. Tumor nests are surrounded by inflammatory cells. The foamy cells are regarded as a reaction to liquefactive necrosis. c Another section of the same case. Scattered tumor cells show vacuolation of the cytoplasm and nuclei, and are surrounded by marked fibrosis
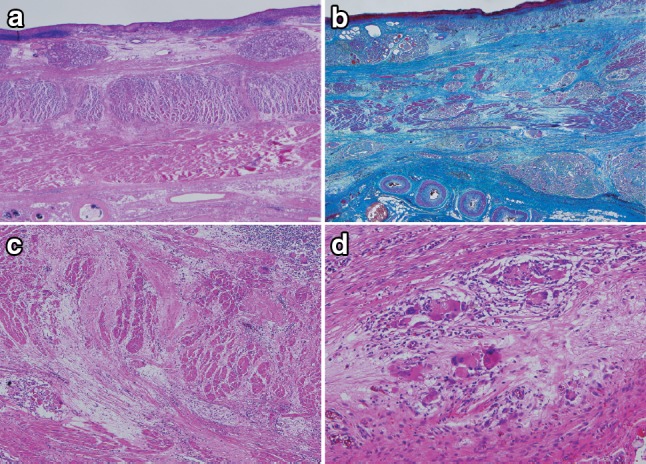
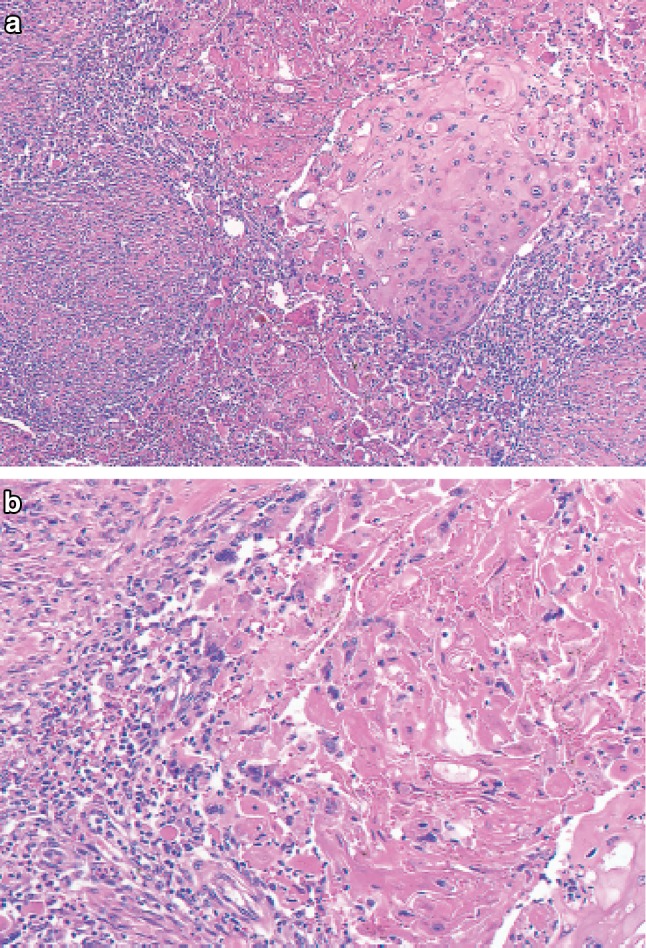
Grade 3: Markedly effective. a Marked fibrosis is noted beneath the squamous epithelium. b Masson staining reveals partial disruption of muscular layer. Fibrosis is noted throughout the esophageal wall. The extent of fibrosis can be regarded as the extent of the preexisting tumor. c Disruption of the muscularis propria and fibrosis are noted. d No viable cancer cell is observed, while foreign body giant cells are scattered. The therapeutic effect is evaluated as grade 3
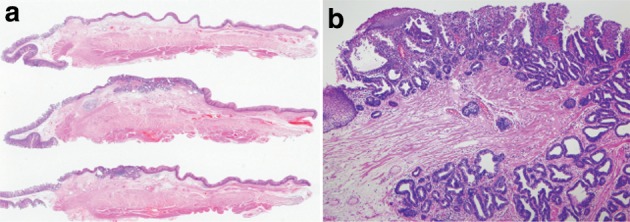
a Barrett esophagus and adenocarcinoma in Barrett esophagus, 0-IIb. The squamocolumnar junction shows an irregularity, with a tongue-like extension of the columnar-lined mucosa towards the esophagus. b Iodine-stained specimen. Iodine staining clearly shows a tongue-like extension of columnar-lined mucosa measuring 30 mm (short segment Barrett esophagus: SSBE). Cancerous lesion was detected pathologically in Barrett mucosa, but it is not visible macroscopically. 0-IIb, pT1a-SMM
Barrett esophagus (specialized columnar epithelium): the esophagus is covered by specialized columnar epithelium with intestinal metaplasia. Squamous epithelium is visible on the distal side (squamous island)
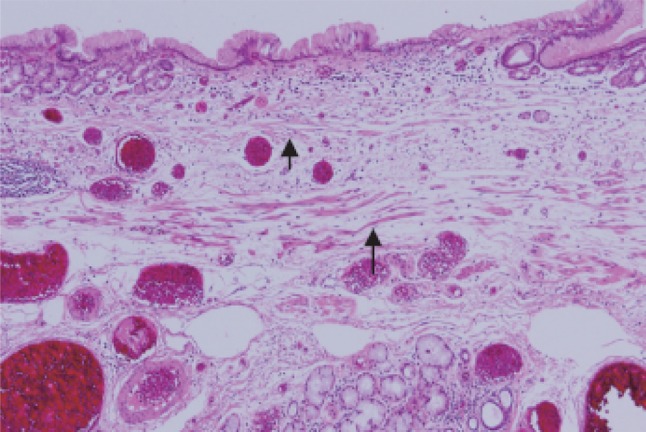
Barrett esophagus (junctional type): a double-layered muscularis mucosae (arrows) is present beneath the overlying columnar epithelium. Esophageal glands are also observed in the submucosal layer. Overlying columnar epithelium is of the cardiac gland type
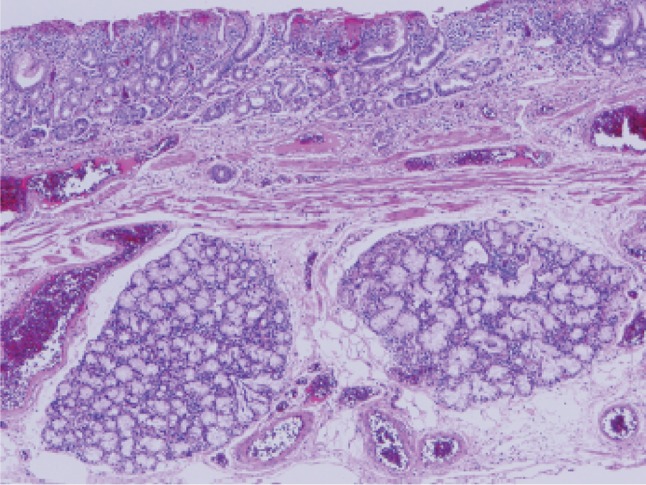
Barrett esophagus (gastric fundic type): the mucosa consists of fundic gland type columnar epithelium. Esophageal glands are observed in the submucosal layer
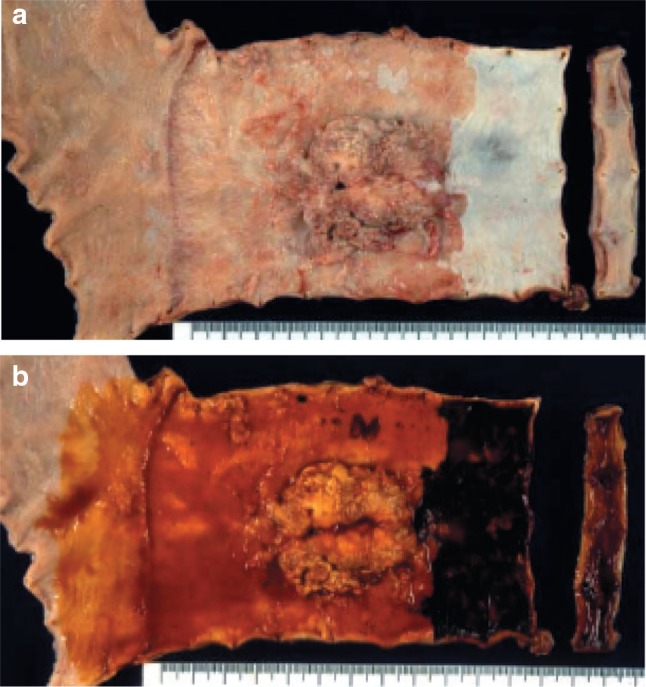
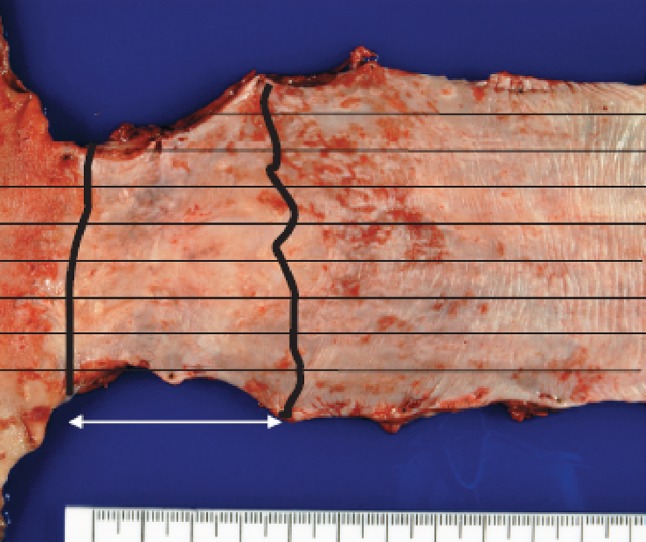
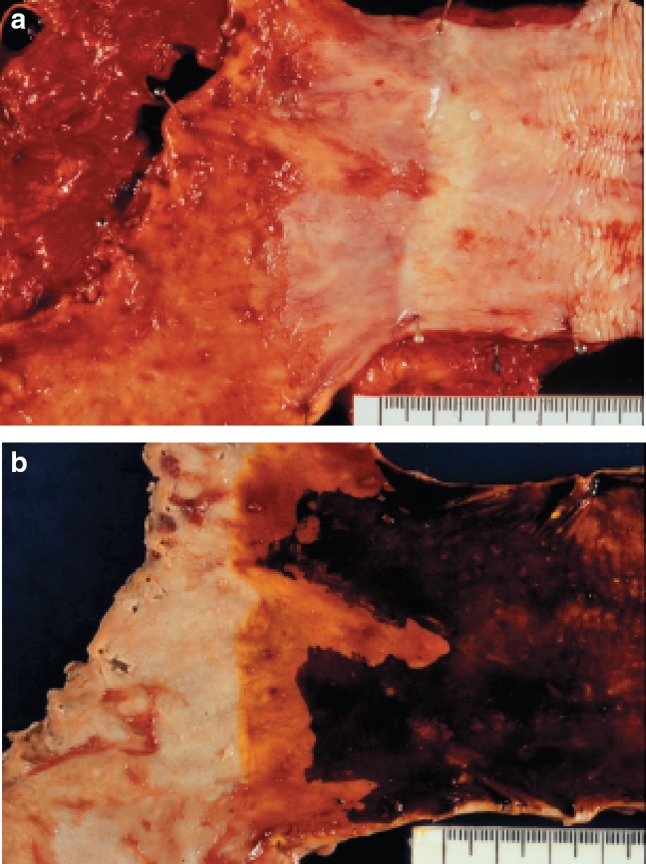
a Adenocarcinoma in Barrett esophagus. Grossly type 1. A section of columnar epithelium measuring 85 mm in length and continuously extending to the esophagus is regarded as long segment Barrett esophagus. A protruding tumor (Type 1) is visible within the section of Barrett esophagus. b Iodine-stained specimen shown in a. Iodine staining clearly reveals the area of Barrett mucosa with scattered iodine-stained squamous islands. The depth of tumor invasion is pT1b
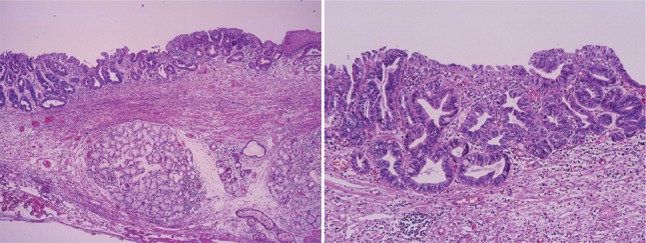
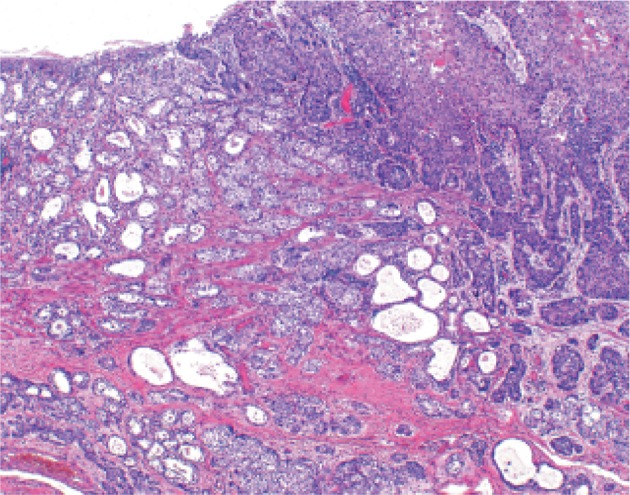
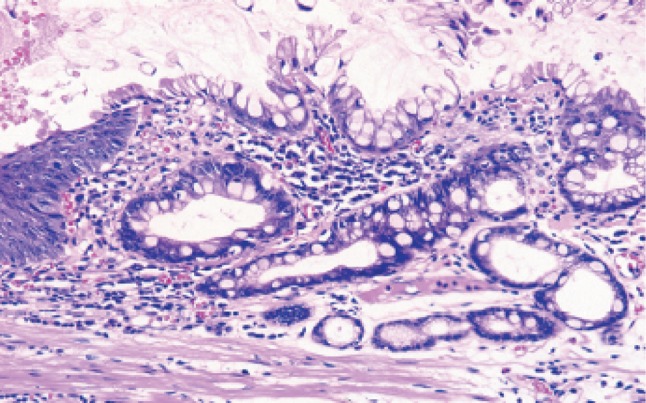
Adenocarcinoma in Barrett esophagus. Barrett esophagus with esophageal glands in the submucosal layer is covered with well differentiated adenocarcinoma. The tumor has invaded beyond the superficial muscularis mucosae, but has not reached the original (deep) muscularis mucosae. Therefore, the depth of tumor invasion should be assessed as pT1a-LPM
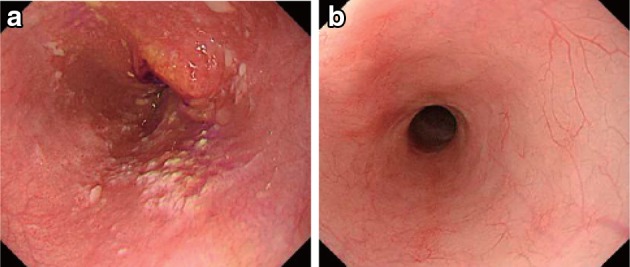
Endoscopic findings of CR cases. a Before treatment: Type 3, cStage IV. b After treatment (5 months after CRT): scarring and mild stenosis are visible. The endoscope could be passed through the entire length of the esophagus. This case was judged as a CR
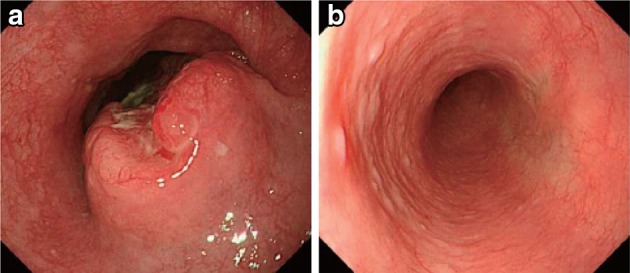
a Before treatment: Type 2, cStage III. b After treatment (chemotherapy): The tumor has disappeared and only a scar remains. This case was judged as a CR
a Before treatment: Type 2, cStage III. b After treatment (6 months after CRT): the tumor has disappeared, and only a scar remains. c After treatment (6 months after CRT): the esophageal mucosa has been stained brown. No unstained areas are present. An endoscopic biopsy from the area of the primary tumor was negative

Iodine staining after treatment. The esophageal mucosa was stained unevenly by the iodine. Some areas stained poorly, while others are dark brown. An endoscopic biopsy was negative, strongly suggesting a CR
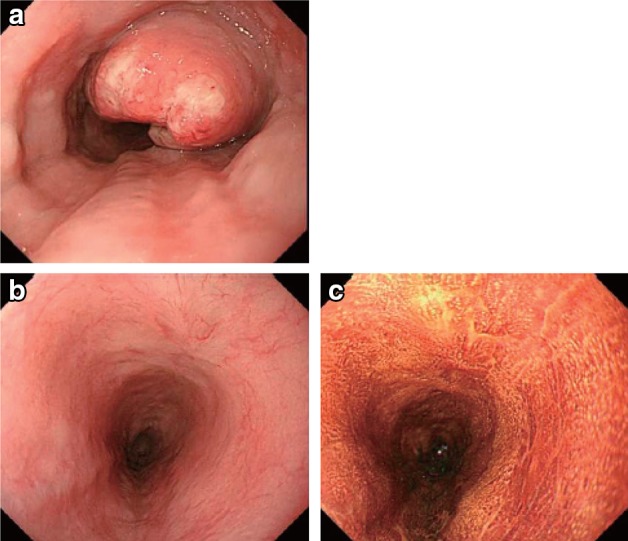
Endoscopic findings of IR/SD cases. a Before treatment: Type 2, cStage III. b, c After treatment (1 month after CRT): an ulcer remains
a Before treatment: Type 2, cStage IVa. b After treatment (CRT): the primary tumor has disappeared. A slightly depressed change surrounded by a marginal elevation is still present. c Narrow band imaging after treatment (CRT) shows a brownish area at the anal margin. d Iodine staining after treatment (CRT): the brownish area was identified as an unstained area. An endoscopic biopsy was positive for malignant cells
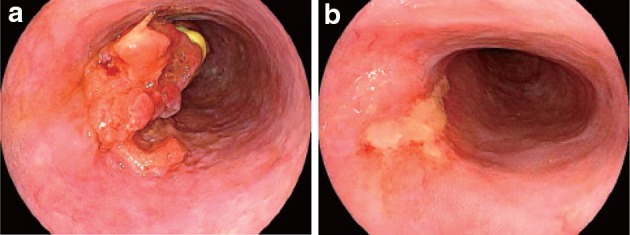
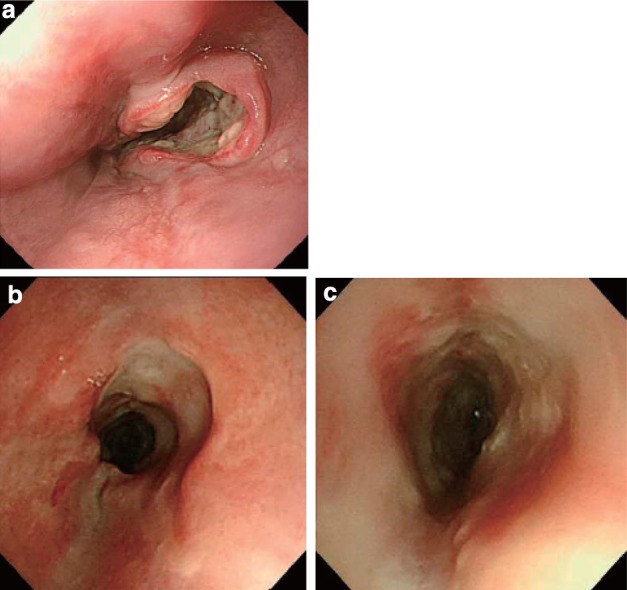
Endoscopic findings of PR cases. a Before treatment: Type 1 + 0-IIc cStage III. b After treatment (2 months after CRT): a marked tumor reduction is visible, although an ulcer with a marginal elevation is present
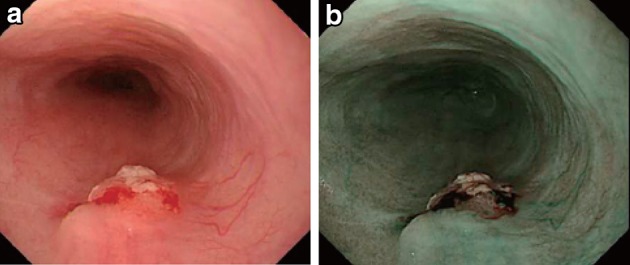
a After treatment (3 months after CRT): a residual tumor was strongly suggested by the presence of a submucosal tumor-like protrusion. Cancer tissue is probably exposed on the top and distal half of the tumor. b The exposed tumor was identified as a brownish area with a central white coating using narrow band imaging
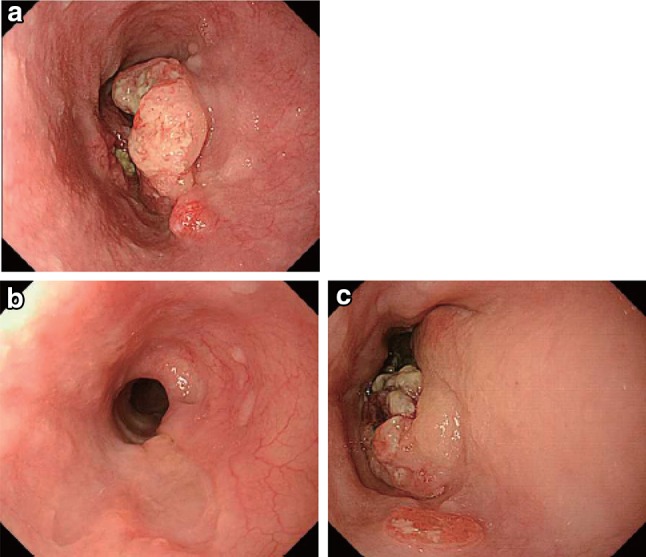
Endoscopic findings of a PD case. a Before treatment: Type 2, cStage III. b After treatment (2 months after CRT): the primary tumor has mostly disappeared. c After treatment (5 months after CRT): the relapsed tumor has increased in size
LinkOut - more resources
Full Text Sources
Other Literature Sources