

Potentially high-risk medication categories and unplanned hospitalizations: a case-time-control study
- PMID: 28112193
- PMCID: PMC5253626
- DOI: 10.1038/srep41035
Potentially high-risk medication categories and unplanned hospitalizations: a case-time-control study
Abstract
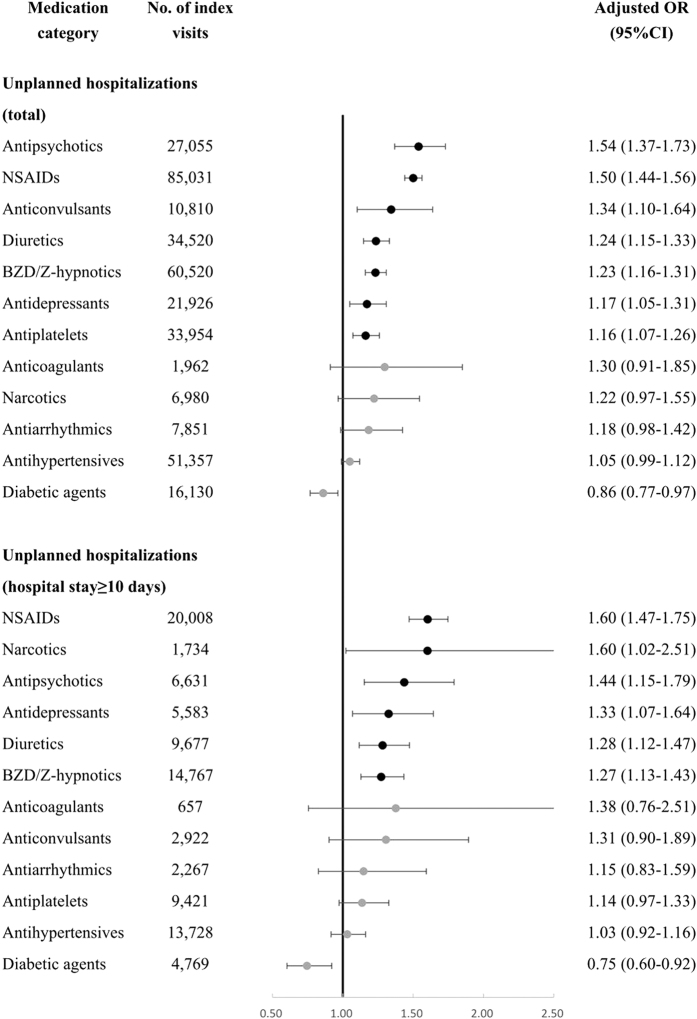
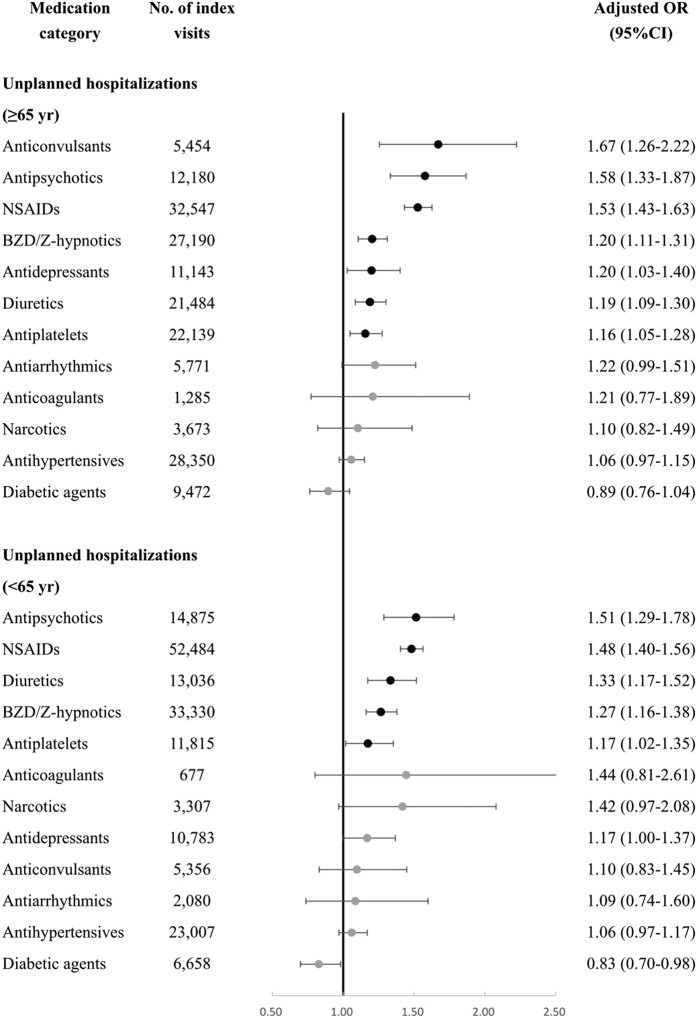
Empirical data of medication-related hospitalization are very limited. We aimed to investigate the associations between 12 high risk medication categories (diabetic agents, diuretics, nonsteroidal anti-inflammatory drugs (NSAIDs), anticoagulants, antiplatelets, antihypertensives, antiarrhythmics, anticonvulsants, antipsychotics, antidepressants, benzodiazepine (BZD)/Z-hypnotics, and narcotics) and unplanned hospitalizations. A population-based case-time-control study was performed using Taiwan's National Health Insurance Research Database. Patients who experienced an unplanned hospitalization (index visit) were identified as index subjects and matched to a randomly selected reference visit within users of a specific category of high-risk medication. An unplanned hospitalization was defined as a hospital admission immediately after an emergency department visit. Discordant exposures to the high-risk medication during the case period (1-14 days before the visit) and the control period (366-379 days before the visit) were examined in both index and reference visits. Antipsychotics was associated with the highest risk of unplanned hospitalizations (adjusted OR: 1.54, 95% CI [1.37-1.73]), followed by NSAIDs (1.50, [1.44-1.56]), anticonvulsants (1.34, [1.10-1.64]), diuretics (1.24, [1.15-1.33]), BZD/Z-hypnotics (1.23, [1.16-1.31]), antidepressants (1.17, [1.05-1.31]) and antiplatelets (1.16, [1.07-1.26]). NSAIDs and narcotics were associated with the highest risks of unplanned hospitalizations with a length of stay ≥10 days. These medication categories should be targeted for clinical and policy interventions.
Figures
References
-
- Nebeker J. R., Barach P. & Samore M. H. Clarifying adverse drug events: a clinician’s guide to terminology, documentation, and reporting. Ann Intern Med. 140, 795–801 (2004). - PubMed
-
- Rottenkolber D. et al.. Adverse drug reactions in Germany: direct costs of internal medicine hospitalizations. Pharmacoepidemiol Drug Saf. 20, 626–634 (2011). - PubMed
-
- Tache S. V., Sonnichsen A. & Ashcroft D. M. Prevalence of adverse drug events in ambulatory care: a systematic review. Ann Pharmacother. 45, 977–989 (2011). - PubMed
-
- Budnitz D. S. et al.. National surveillance of emergency department visits for outpatient adverse drug events. JAMA. 296, 1858–1866 (2006). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
