

Cardiac Toxicity After Radiotherapy for Stage III Non-Small-Cell Lung Cancer: Pooled Analysis of Dose-Escalation Trials Delivering 70 to 90 Gy
- PMID: 28113017
- PMCID: PMC5455462
- DOI: 10.1200/JCO.2016.70.0229
Cardiac Toxicity After Radiotherapy for Stage III Non-Small-Cell Lung Cancer: Pooled Analysis of Dose-Escalation Trials Delivering 70 to 90 Gy
Abstract
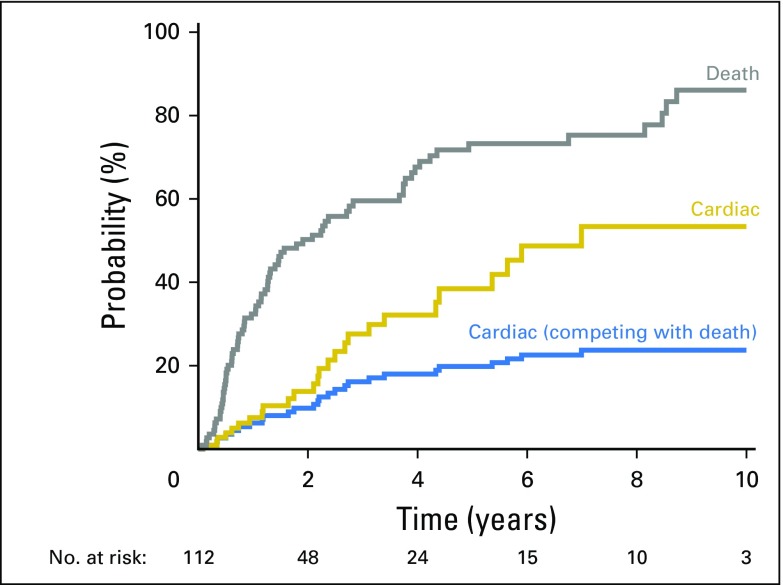
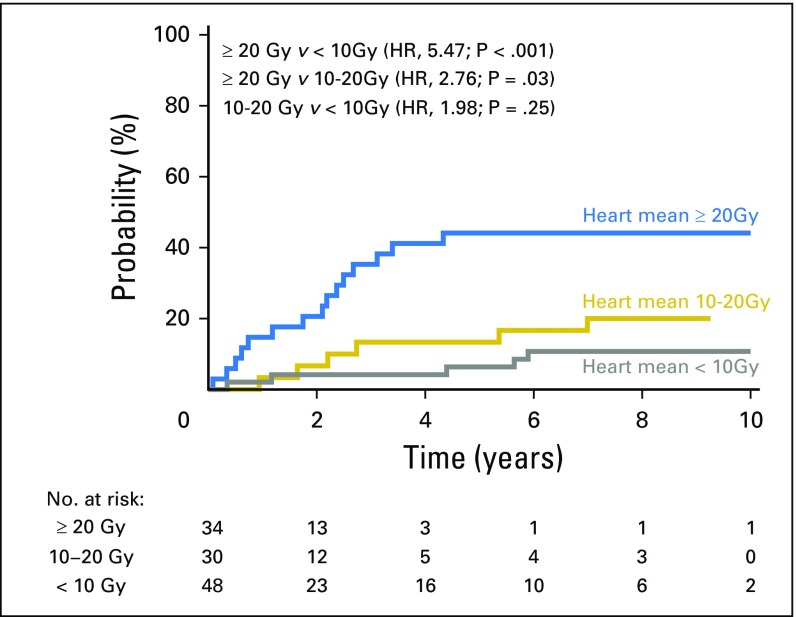
Purpose The significance of radiotherapy (RT) -associated cardiac injury for stage III non-small-cell lung cancer (NSCLC) is unclear, but higher heart doses were associated with worse overall survival in the Radiation Therapy Oncology Group (RTOG) 0617 study. We assessed the impact of heart dose in patients treated at our institution on several prospective dose-escalation trials. Patients and Methods From 1996 to 2009, 127 patients with stage III NSCLC (Eastern Cooperative Oncology Group performance status, 0 to 1) received dose-escalated RT to 70 to 90 Gy (median, 74 Gy) in six trials. RT plans and cardiac doses were reviewed. Records were reviewed for the primary end point: symptomatic cardiac events (symptomatic pericardial effusion, acute coronary syndrome, pericarditis, significant arrhythmia, and heart failure). Cardiac risk was assessed by noting baseline coronary artery disease and calculating the WHO/International Society of Hypertension score. Competing risks analysis was used. Results In all, 112 patients were analyzed. Median follow-up for surviving patients was 8.8 years. Twenty-six patients (23%) had one or more events at a median of 26 months to first event (effusion [n = 7], myocardial infarction [n = 5], unstable angina [n = 3], pericarditis [n = 2], arrhythmia [n = 12], and heart failure [n = 1]). Heart doses (eg, heart mean dose; hazard ratio, 1.03/Gy; P = .002,), coronary artery disease ( P < .001), and WHO/International Society of Hypertension score ( P = .04) were associated with events on univariable analysis. Heart doses remained significant on multivariable analysis that accounted for baseline risk. Two-year competing risk-adjusted event rates for patients with heart mean dose < 10 Gy, 10 to 20 Gy, or ≥ 20 Gy were 4%, 7%, and 21%, respectively. Heart doses were not associated with overall survival. Conclusion Cardiac events were relatively common after high-dose thoracic RT and were independently associated with both heart dose and baseline cardiac risk. RT-associated cardiac toxicity after treatment of stage III NSCLC may occur earlier than historically understood, and heart doses should be minimized.
Figures
Comment in
-
New Era in Radiation Oncology for Lung Cancer: Recognizing the Importance of Cardiac Irradiation.J Clin Oncol. 2017 May 1;35(13):1381-1383. doi: 10.1200/JCO.2016.71.5581. Epub 2017 Jan 23. J Clin Oncol. 2017. PMID: 28113024 No abstract available.
-
Getting to the Heart of the Matter: What Additional Proof Is Needed to Demonstrate the Value of Intensity-Modulated Radiotherapy in Thoracic Oncology?J Clin Oncol. 2017 Jul 1;35(19):2215-2216. doi: 10.1200/JCO.2017.73.1786. Epub 2017 May 8. J Clin Oncol. 2017. PMID: 28481710 No abstract available.
-
Locally Advanced Lung Cancer: Is It Time to Take Cardiac Protection Seriously in Radiation Planning?Int J Radiat Oncol Biol Phys. 2018 Apr 1;100(5):1091-1094. doi: 10.1016/j.ijrobp.2017.09.044. Int J Radiat Oncol Biol Phys. 2018. PMID: 29722650 No abstract available.
References
-
- Cuzick J, Stewart H, Rutqvist L, et al. Cause-specific mortality in long-term survivors of breast cancer who participated in trials of radiotherapy. J Clin Oncol. 1994;12:447–453. - PubMed
-
- Darby SC, McGale P, Taylor CW, et al. Long-term mortality from heart disease and lung cancer after radiotherapy for early breast cancer: Prospective cohort study of about 300,000 women in US SEER cancer registries. Lancet Oncol. 2005;6:557–565. - PubMed
-
- Hooning MJ, Botma A, Aleman BM, et al. Long-term risk of cardiovascular disease in 10-year survivors of breast cancer. J Natl Cancer Inst. 2007;99:365–375. - PubMed
-
- van Nimwegen FA, Schaapveld M, Janus CP, et al. Cardiovascular disease after Hodgkin lymphoma treatment: 40-year disease risk. JAMA Intern Med. 2015;175:1007–1017. - PubMed
-
- van Nimwegen FA, Schaapveld M, Cutter DJ, et al. Radiation dose-response relationship for risk of coronary heart disease in survivors of Hodgkin lymphoma. J Clin Oncol. 2016;34:235–243. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
