

Association of Delayed Antimicrobial Therapy with One-Year Mortality in Pediatric Sepsis
- PMID: 28114166
- PMCID: PMC5468469
- DOI: 10.1097/SHK.0000000000000833
Association of Delayed Antimicrobial Therapy with One-Year Mortality in Pediatric Sepsis
Abstract
Objective: Delayed antimicrobial therapy in sepsis is associated with increased hospital mortality, but the impact of antimicrobial timing on long-term outcomes is unknown. We tested the hypothesis that hourly delays to antimicrobial therapy are associated with 1-year mortality in pediatric severe sepsis.
Design: Retrospective observational study.
Setting: Quaternary academic pediatric intensive care unit (PICU) from February 1, 2012 to June 30, 2013.
Patients: One hundred sixty patients aged ≤21 years treated for severe sepsis.
Interventions: None.
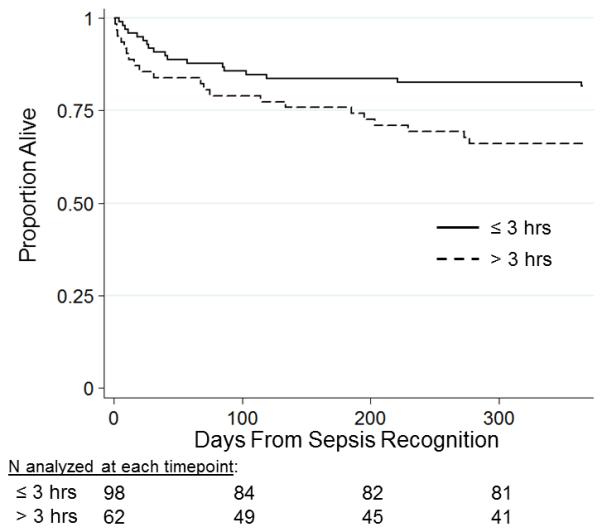
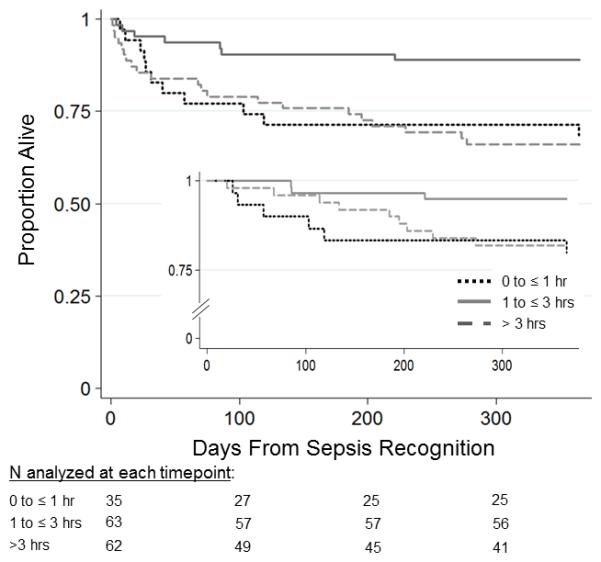
Measurements and main results: We tested the association of hourly delays from sepsis recognition to antimicrobial administration with 1-year mortality using multivariable Cox and logistic regression. Overall 1-year mortality was 24% (39 patients), of whom 46% died after index PICU discharge. Median time from sepsis recognition to antimicrobial therapy was 137 min (IQR 65-287). After adjusting for severity of illness and comorbid conditions, hourly delays up to 3 h were not associated with 1-year mortality. However, increased 1-year mortality was evident in patients who received antimicrobials ≤1 h (aOR 3.8, 95% CI 1.2, 11.7) or >3 h (aOR 3.5, 95% CI 1.3, 9.8) compared with patients who received antimicrobials within 1 to 3 h from sepsis recognition. For the subset of patients who survived index PICU admission, antimicrobial therapy ≤1 h was also associated with increased 1-year mortality (aOR 5.5, 95% CI 1.1, 27.4), while antimicrobial therapy >3 h was not associated with 1-year mortality (aOR 2.2, 95% CI 0.5, 11.0).
Conclusions: Hourly delays to antimicrobial therapy, up to 3 h, were not associated with 1-year mortality in pediatric severe sepsis in this study. The finding that antimicrobial therapy ≤1 h from sepsis recognition was associated with increased 1-year mortality should be regarded as hypothesis-generating for future studies.
Figures
References
-
- Hartman ME, Linde-Zwirble WT, Angus DC, Watson RS. Trends in the epidemiology of pediatric severe sepsis. Pediatr Crit Care Med. 2013;14(7):686–93. - PubMed
-
- Weiss SL, Fitzgerald JC, Pappachan J, Wheeler D, Jaramillo-Bustamante JC, Salloo A, Singhi SC, Erickson S, Roy JA, Bush JL, Nadkarni VM, Thomas NJ. Global epidemiology of pediatric severe sepsis: the sepsis prevalence, outcomes, and therapies study. Am J Respir Crit Care Med. 2015;191(10):1147–57. - PMC - PubMed
-
- Jaramillo-Bustamante JC, Marin-Agudelo A, Fernandez-Laverde M, Bareno-Silva J. Epidemiology of sepsis in pediatric intensive care units: first Colombian multicenter study. Pediatr Crit Care Med. 2012;13(5):501–8. - PubMed
-
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb SA, Beale RJ, Vincent JL, Moreno R. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637. - PubMed
-
- Ferrer R, Artigas A, Suarez D, Palencia E, Levy MM, Arenzana A, Perez XL, Sirvent JM. Effectiveness of treatments for severe sepsis: a prospective, multicenter, observational study. Am J Respir Crit Care Med. 2009;180(9):861–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
