

Association of Delirium With Cognitive Decline in Late Life: A Neuropathologic Study of 3 Population-Based Cohort Studies
- PMID: 28114436
- PMCID: PMC6037291
- DOI: 10.1001/jamapsychiatry.2016.3423
Association of Delirium With Cognitive Decline in Late Life: A Neuropathologic Study of 3 Population-Based Cohort Studies
Abstract
Importance: Delirium is associated with accelerated cognitive decline. The pathologic substrates of this association are not yet known, that is, whether they are the same as those associated with dementia, are independent, or are interrelated.
Objective: To examine whether the accelerated cognitive decline observed after delirium is independent of the pathologic processes of classic dementia.
Design, setting, and participants: Harmonized data from 987 individual brain donors from 3 observational cohort studies with population-based sampling (Vantaa 85+, Cambridge City Over-75s Cohort, Cognitive Function and Ageing Study) performed from January 1, 1985, through December 31, 2011, with a median follow-up of 5.2 years until death, were used in this study. Neuropathologic assessments were performed with investigators masked to clinical data. Data analysis was performed from January 1, 2012, through December 31, 2013. Clinical characteristics of brain donors were not different from the rest of the cohort. Outcome ascertainment was complete given that the participants were brain donors.
Exposures: Delirium (never vs ever) and pathologic burden of neurofibrillary tangles, amyloid plaques, vascular lesions, and Lewy bodies. Effects modeled using random-effects linear regression and interactions between delirium and pathologic burden were assessed.
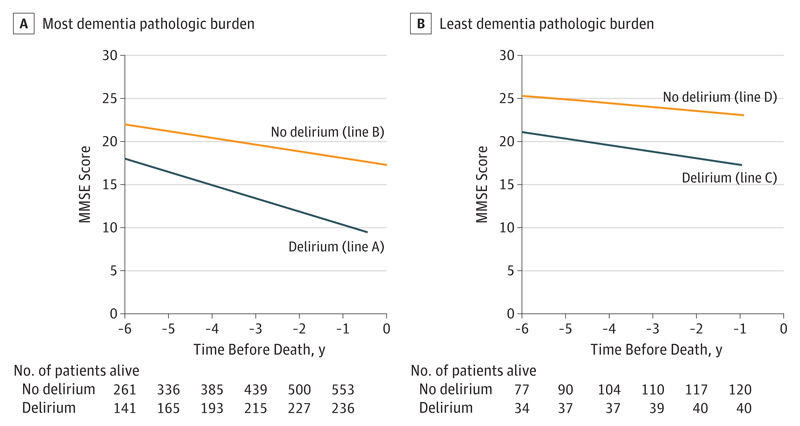
Outcomes: Change in Mini-Mental State Examination (MMSE) scores during the 6 years before death.
Results: There were 987 participants (290 from Vantaa 85+, 241 from the Cambridge City Over-75s Cohort, and 456 from the Cognitive Function and Ageing Study) with neuropathologic data; mean (SD) age at death was 90 (6.4) years, including 682 women (69%). The mean MMSE score 6 years before death was 24.7 points. The 279 individuals with delirium (75% women) had worse initial scores (-2.8 points; 95% CI, -4.5 to -1.0; P < .001). Cognitive decline attributable to delirium was -0.37 MMSE points per year (95% CI, -0.60 to -0.13; P < .001). Decline attributable to the pathologic processes of dementia was -0.39 MMSE points per year (95% CI, -0.57 to -0.22; P < .001). However, the combination of delirium and the pathologic processes of dementia resulted in the greatest decline, in which the interaction contributed an additional -0.16 MMSE points per year (95% CI, -0.29 to -0.03; P = .01). The multiplicative nature of these variables resulted in individuals with delirium and the pathologic processes of dementia declining 0.72 MMSE points per year faster than age-, sex-, and educational level-matched controls.
Conclusions and relevance: Delirium in the presence of the pathologic processes of dementia is associated with accelerated cognitive decline beyond that expected for delirium or the pathologic process itself. These findings suggest that additional unmeasured pathologic processes specifically relate to delirium. Age-related cognitive decline has many contributors, and these findings at the population level support a role for delirium acting independently and multiplicatively to the pathologic processes of classic dementia.
Conflict of interest statement
Figures
Comment in
-
Delirium, Dementia, and Decline.JAMA Psychiatry. 2017 Mar 1;74(3):212-213. doi: 10.1001/jamapsychiatry.2016.3812. JAMA Psychiatry. 2017. PMID: 28114516 No abstract available.
References
-
- Savva GM, Wharton SB, Ince PG, Forster G, Matthews FE, Brayne C, Medical Research Council Cognitive Function and Ageing Study Age, neuropathology, and dementia. N Engl J Med. 2009;360(22):2302–2309. - PubMed
-
- Siddiqi N, House AO, Holmes JD. Occurrence and outcome of delirium in medical in-patients: a systematic literature review. Age Ageing. 2006;35(4):350–364. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
