

Procalcitonin-guided diagnosis and antibiotic stewardship revisited
- PMID: 28114931
- PMCID: PMC5259962
- DOI: 10.1186/s12916-017-0795-7
Procalcitonin-guided diagnosis and antibiotic stewardship revisited
Abstract
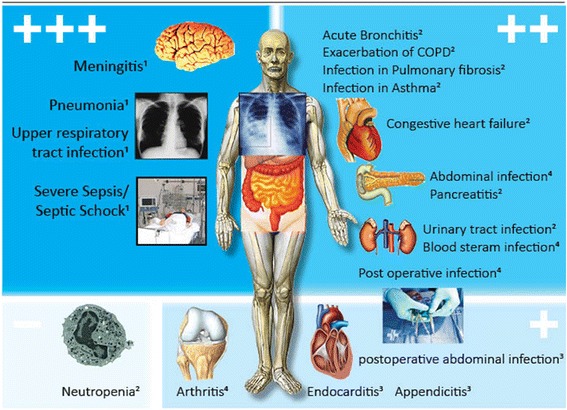
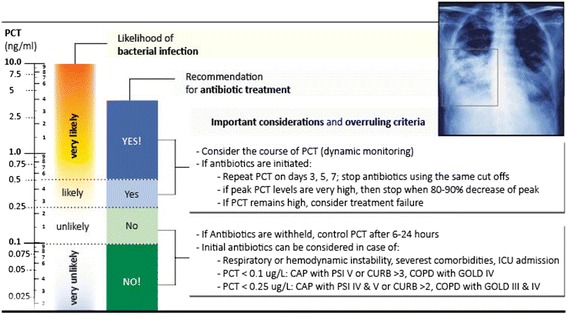
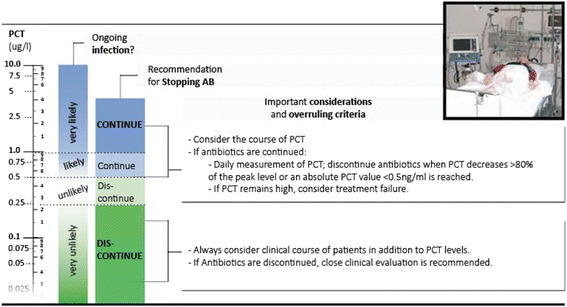
Several controlled clinical studies have evaluated the potential of the infection biomarker procalcitonin (PCT) to improve the diagnostic work-up of patients with bacterial infections and its influence on decisions regarding antibiotic therapy. Most research has focused on lower respiratory tract infections and critically ill sepsis patients. A clinical utility for PCT has also been found for patients with urinary tract infections, postoperative infections, meningitis, and patients with acute heart failure with possible superinfection (i.e., pneumonia). In these indications, PCT levels measured on hospital admission were found to substantially reduce the initiation of antibiotic treatment in low-risk situations (i.e., bronchitis, chronic obstructive pulmonary disease exacerbation). For more severe infections (i.e., pneumonia, sepsis), antibiotic stewardship by monitoring of PCT kinetics resulted in shorter antibiotic treatment durations with early cessation of therapy. Importantly, these strategies appear to be safe without increasing the risk for mortality, recurrent infections, or treatment failures. PCT kinetics also proved to have prognostic value correlating with disease severity (i.e., pancreatitis, abdominal infection) and resolution of illness (i.e., sepsis). Although promising findings have been published in these different types of infections, there are a number of limitations regarding PCT, including suboptimal sensitivity and/or specificity, which makes a careful interpretation of PCT in the clinical context mandatory. This narrative review aims to update clinicians on the strengths and limitations of PCT for patient management, focusing on research conducted within the last 4 years.
Keywords: Antibiotic stewardship; Pneumonia; Procalcitonin; Respiratory tract infection; Sepsis.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
