

Physician Assessment of Pretest Probability of Malignancy and Adherence With Guidelines for Pulmonary Nodule Evaluation
- PMID: 28115167
- PMCID: PMC6026222
- DOI: 10.1016/j.chest.2017.01.018
Physician Assessment of Pretest Probability of Malignancy and Adherence With Guidelines for Pulmonary Nodule Evaluation
Abstract
Background: The annual incidence of pulmonary nodules is estimated at 1.57 million. Guidelines recommend using an initial assessment of nodule probability of malignancy (pCA). A previous study found that despite this recommendation, physicians did not follow guidelines.
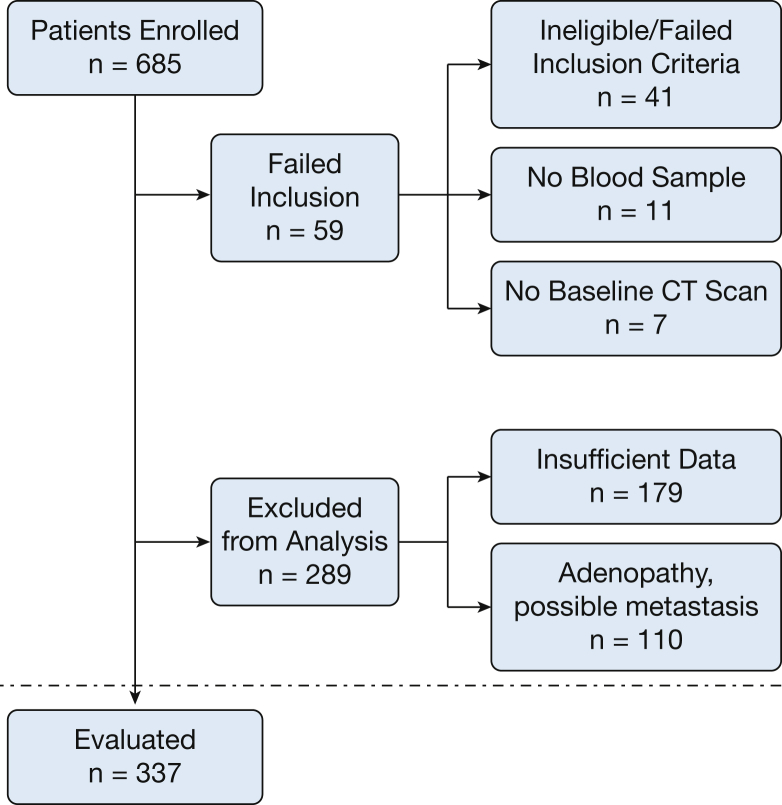
Methods: Physician assessments (N = 337) and two previously validated risk model assessments of pretest probability of cancer were evaluated for performance in 337 patients with pulmonary nodules based on final diagnosis and compared. Physician-assessed pCA was categorized into low, intermediate, and high risk, and the next test ordered was evaluated.
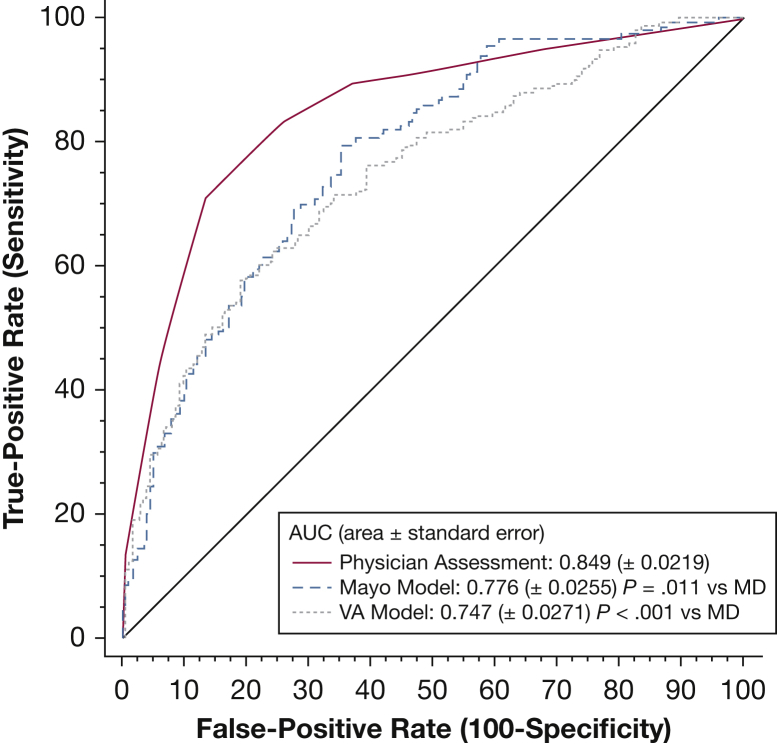
Results: The prevalence of malignancy was 47% (n = 158) at 1 year. Physician-assessed pCA performed better than nodule prediction calculators (area under the curve, 0.85 vs 0.75; P < .001 and .78; P = .0001). Physicians did not follow indicated guidelines when selecting the next test in 61% of cases (n = 205). Despite recommendations for serial CT imaging in those with low pCA, 52% (n = 13) were managed more aggressively with PET imaging or biopsy; 12% (n = 3) underwent biopsy procedures for benign disease. Alternatively, in the high-risk category, the majority (n = 103 [75%]) were managed more conservatively. Stratified by diagnosis, 92% (n = 22) with benign disease underwent more conservative management with CT imaging (20%), PET scanning (15%), or biopsy (8%), although three had surgery (8%).
Conclusions: Physician assessment as a means for predicting malignancy in pulmonary nodules is more accurate than previously validated nodule prediction calculators. Despite the accuracy of clinical intuition, physicians did not follow guideline-based recommendations when selecting the next diagnostic test. To provide optimal patient care, focus in the areas of guideline refinement, implementation, and dissemination is needed.
Keywords: guideline adherence; nodule management; nodule risk prediction; pulmonary nodules.
Published by Elsevier Inc.
Figures
Comment in
-
Pulmonary Nodule Guidelines: What Physicians Do When Evidence-Based Guidelines Lack High-Quality Evidence.Chest. 2017 Aug;152(2):232-234. doi: 10.1016/j.chest.2017.03.009. Chest. 2017. PMID: 28797383 No abstract available.
-
Physician Assessment of Pretest Probability of Malignancy and Adherence to Guidelines for Pulmonary Nodule Evaluation.Chest. 2017 Aug;152(2):447-448. doi: 10.1016/j.chest.2017.03.045. Chest. 2017. PMID: 28797389 No abstract available.
-
Response.Chest. 2017 Aug;152(2):448-449. doi: 10.1016/j.chest.2017.03.043. Chest. 2017. PMID: 28797390 No abstract available.
References
-
- Gould M.K., Tang T., Liu I.L. Recent trends in the identification of incidental pulmonary nodules. Am J Respir Crit Care Med. 2015;192(10):1208–1214. - PubMed
-
- Baldwin D.R., Callister M.E., Guideline Development Group The British Thoracic Society guidelines on the investigation and management of pulmonary nodules. Thorax. 2015;70(8):794–798. - PubMed
-
- Swensen S.J., Silverstein M.D., Ilstrup D.M., Schleck C.D., Edell E.S. The probability of malignancy in solitary pulmonary nodules. Application to small radiologically indeterminate nodules. Arch Intern Med. 1997;157(8):849–855. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
