

Lack of adherence to SHEA-IDSA treatment guidelines for Clostridium difficile infection is associated with increased mortality
- PMID: 28115504
- PMCID: PMC6074846
- DOI: 10.1093/jac/dkw423
Lack of adherence to SHEA-IDSA treatment guidelines for Clostridium difficile infection is associated with increased mortality
Abstract
Objectives: The objective of this study was to determine our institution's compliance with 2010 Society for Healthcare Epidemiology of America and IDSA Clostridium difficile infection (CDI) treatment guidelines and their respective outcomes.
Methods: We collected clinical parameters, laboratory values, antibiotic therapy and clinical outcomes from the electronic medical records for all patients hospitalized at our institution with a diagnosis of CDI from December 2012 to November 2013. We specifically evaluated whether SHEA-IDSA treatment guidelines were followed and evaluated the associations between guideline adherence and severe outcomes including mortality.
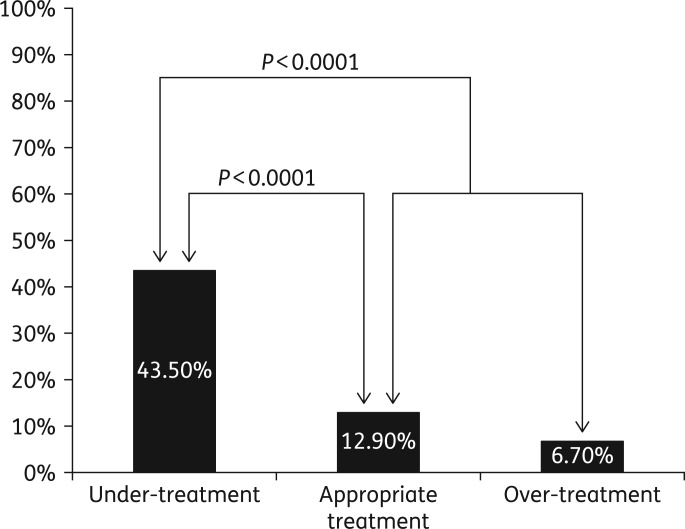
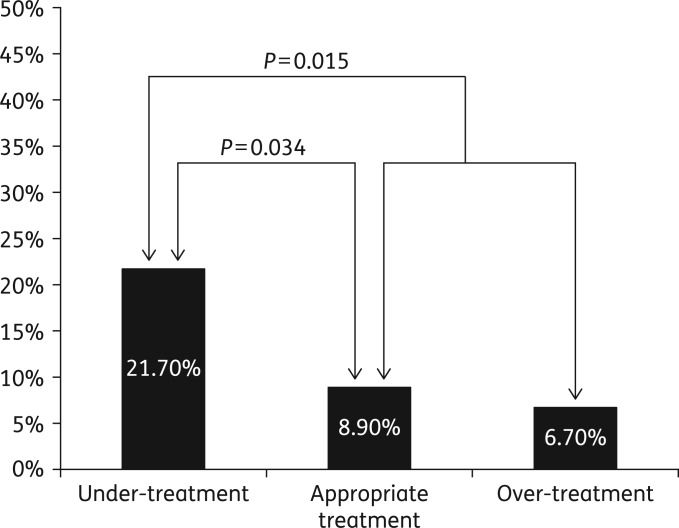
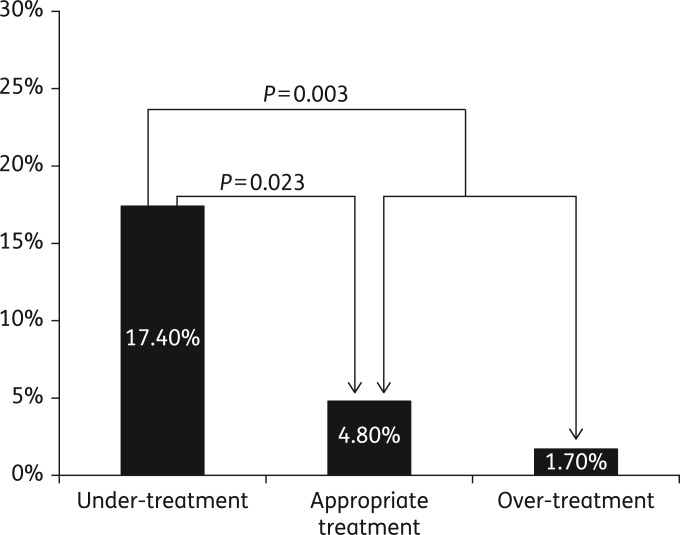
Results: We identified 230 patients with CDI meeting inclusion criteria during the study period. Of these, 124 (54%) were appropriately treated, 46 (20%) were under-treated and 60 (26%) were over-treated. All-cause 90 day mortality was 17.4% overall; 43.5% in the under-treated group versus 12.9% in those appropriately treated (P < 0.0001) and 10.9% in those appropriately treated plus over-treated (P < 0.0001). Similarly, 90 day mortality attributed to CDI was 21.7% in those under-treated versus 8.9% in those appropriately treated (P = 0.03) and 8.2% in those either appropriately treated or over-treated (P = 0.015). Severe-complicated CDI occurred in 46 patients. In this subgroup, there was a non-significant trend towards increased mortality in under-treated patients (56.7%) compared with appropriately treated patients (37.5%, P = 0.35). Under-treatment was also associated with a higher rate of CDI-related ICU transfer (17.4% versus 4.8% in those appropriately treated, P = 0.023).
Conclusions: Adherence to CDI treatment guidelines is associated with improved outcomes especially in those with severe disease. Increased emphasis on provision of appropriate, guideline-based CDI treatment appears warranted.
© The Author 2016. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Kelly CP, LaMont JT. Clostridium difficile—more difficult than ever. New Engl J Med 2008; 359: 1932–40. - PubMed
-
- Kelly CP, Pothoulakis C, LaMont JT. Clostridium difficile colitis. New Engl J Med 1994; 330: 257–62. - PubMed
-
- Bartlett JG. Antibiotic-associated diarrhea. Clin Infect Dis 1992; 15: 573–81. - PubMed
-
- O'Brien JA, Lahue BJ, Caro JJ et al. . The emerging infectious challenge of Clostridium difficile-associated disease in Massachusetts hospitals: clinical and economic consequences. Infect Control Hosp Epidemiol 2007; 28: 1219–27. - PubMed
-
- Miller BA, Chen LF, Sexton DJ et al. . Comparison of the burdens of hospital-onset, healthcare facility-associated Clostridium difficile infection and of healthcare-associated infection due to methicillin-resistant Staphylococcus aureus in community hospitals. Infect Control Hosp Epidemiol 2011; 32: 387–90. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
