

Abnormal Wave Reflections and Left Ventricular Hypertrophy Late After Coarctation of the Aorta Repair
- PMID: 28115510
- PMCID: PMC5295491
- DOI: 10.1161/HYPERTENSIONAHA.116.08763
Abnormal Wave Reflections and Left Ventricular Hypertrophy Late After Coarctation of the Aorta Repair
Abstract
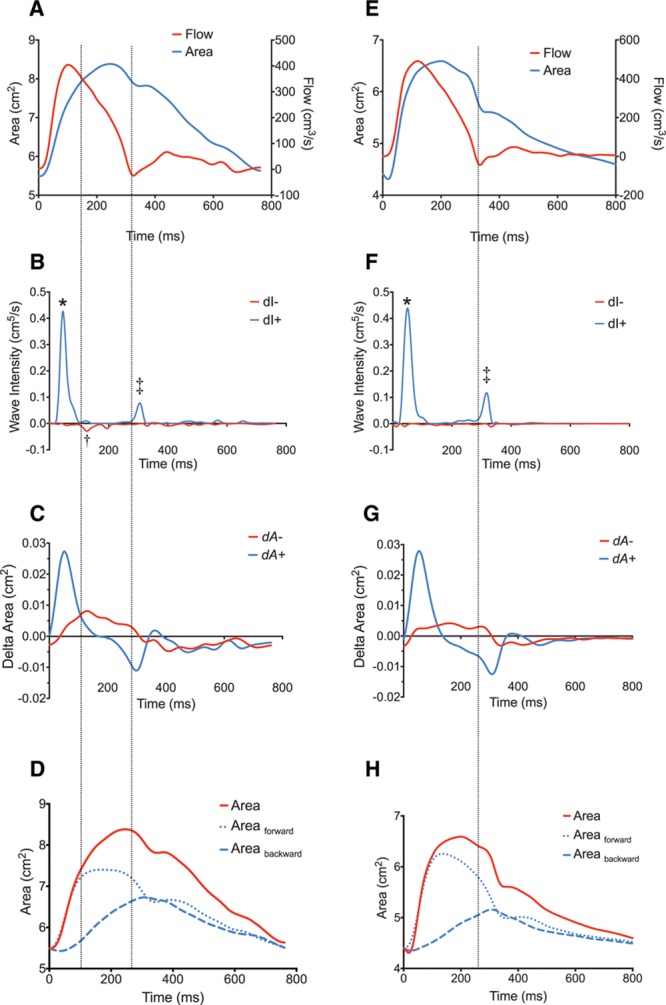
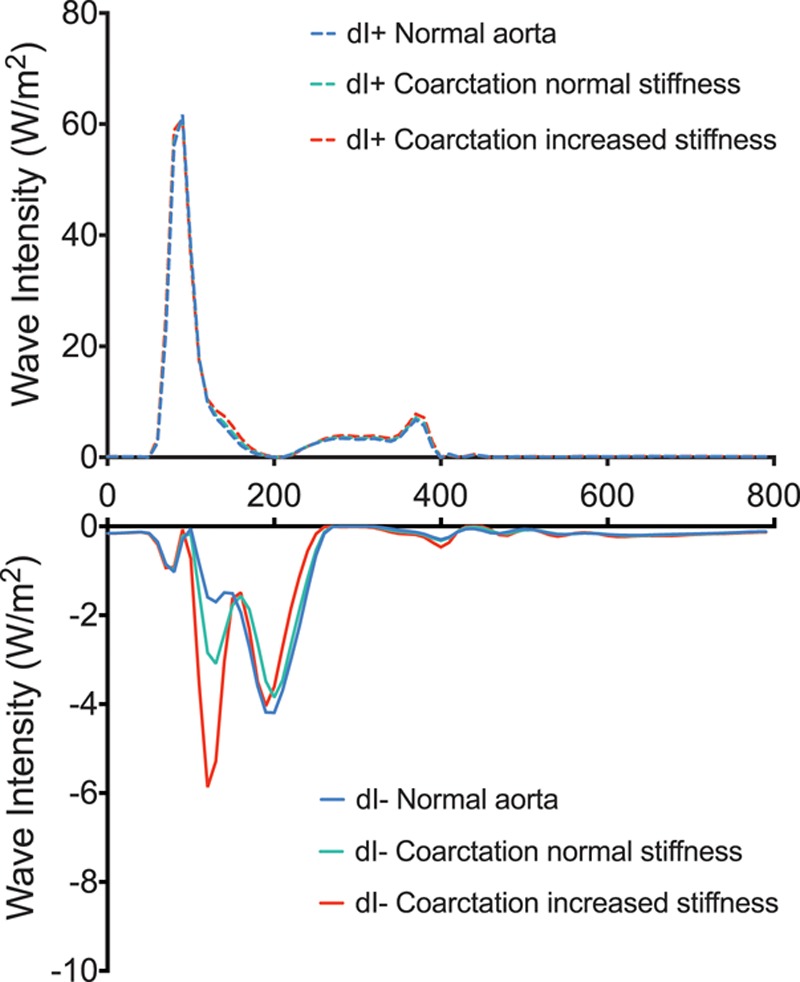
Patients with repaired coarctation of the aorta are thought to have increased afterload due to abnormalities in vessel structure and function. We have developed a novel cardiovascular magnetic resonance protocol that allows assessment of central hemodynamics, including central aortic systolic blood pressure, resistance, total arterial compliance, pulse wave velocity, and wave reflections. The main study aims were to (1) characterize group differences in central aortic systolic blood pressure and peripheral systolic blood pressure, (2) comprehensively evaluate afterload (including wave reflections) in the 2 groups, and (3) identify possible biomarkers among covariates associated with elevated left ventricular mass (LVM). Fifty adult patients with repaired coarctation and 25 age- and sex-matched controls were recruited. Ascending aorta area and flow waveforms were obtained using a high temporal-resolution spiral phase-contrast cardiovascular magnetic resonance flow sequence. These data were used to derive central hemodynamics and to perform wave intensity analysis noninvasively. Covariates associated with LVM were assessed using multivariable linear regression analysis. There were no significant group differences (P≥0.1) in brachial systolic, mean, or diastolic BP. However central aortic systolic blood pressure was significantly higher in patients compared with controls (113 versus 107 mm Hg, P=0.002). Patients had reduced total arterial compliance, increased pulse wave velocity, and larger backward compression waves compared with controls. LVM index was significantly higher in patients than controls (72 versus 59 g/m2, P<0.0005). The magnitude of the backward compression waves was independently associated with variation in LVM (P=0.01). Using a novel, noninvasive hemodynamic assessment, we have shown abnormal conduit vessel function after coarctation of the aorta repair, including abnormal wave reflections that are associated with elevated LVM.
Keywords: blood pressure; congenital heart disease; hemodynamics; hypertension; magnetic resonance imaging.
© 2017 The Authors.
Figures
References
-
- Quail MA, Steeden JA, Knight D, Segers P, Taylor AM, Muthurangu V. Development and validation of a novel method to derive central aortic systolic pressure from the MR aortic distension curve. J Magn Reson Imaging. 2014;40:1064–1070. doi: 10.1002/jmri.24471. - PubMed
-
- Biglino G, Steeden JA, Baker C, Schievano S, Taylor AM, Parker KH, Muthurangu V. A non-invasive clinical application of wave intensity analysis based on ultrahigh temporal resolution phase-contrast cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2012;14:57. doi: 10.1186/1532-429X-14-57. - PMC - PubMed
-
- Muthurangu V, Taylor AM, Hegde SR, Johnson R, Tulloh R, Simpson JM, Qureshi S, Rosenthal E, Baker E, Anderson D, Razavi R. Cardiac magnetic resonance imaging after stage I Norwood operation for hypoplastic left heart syndrome. Circulation. 2005;112:3256–3263. doi: 10.1161/CIRCULATIONAHA.105.543686. - PubMed
Publication types
MeSH terms
Grants and funding
- FS/16/28/32327/BHF_/British Heart Foundation/United Kingdom
- FS/08/012/24454/BHF_/British Heart Foundation/United Kingdom
- FS/11/76/29037/BHF_/British Heart Foundation/United Kingdom
- PG/11/98/29201/BHF_/British Heart Foundation/United Kingdom
- PG/10/76/28545/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
