

The impact of HIV and antiretroviral therapy on TB risk in children: a systematic review and meta-analysis
- PMID: 28115682
- PMCID: PMC5520282
- DOI: 10.1136/thoraxjnl-2016-209421
The impact of HIV and antiretroviral therapy on TB risk in children: a systematic review and meta-analysis
Abstract
Background: Children (<15 years) are vulnerable to TB disease following infection, but no systematic review or meta-analysis has quantified the effects of HIV-related immunosuppression or antiretroviral therapy (ART) on their TB incidence.
Objectives: Determine the impact of HIV infection and ART on risk of incident TB disease in children.
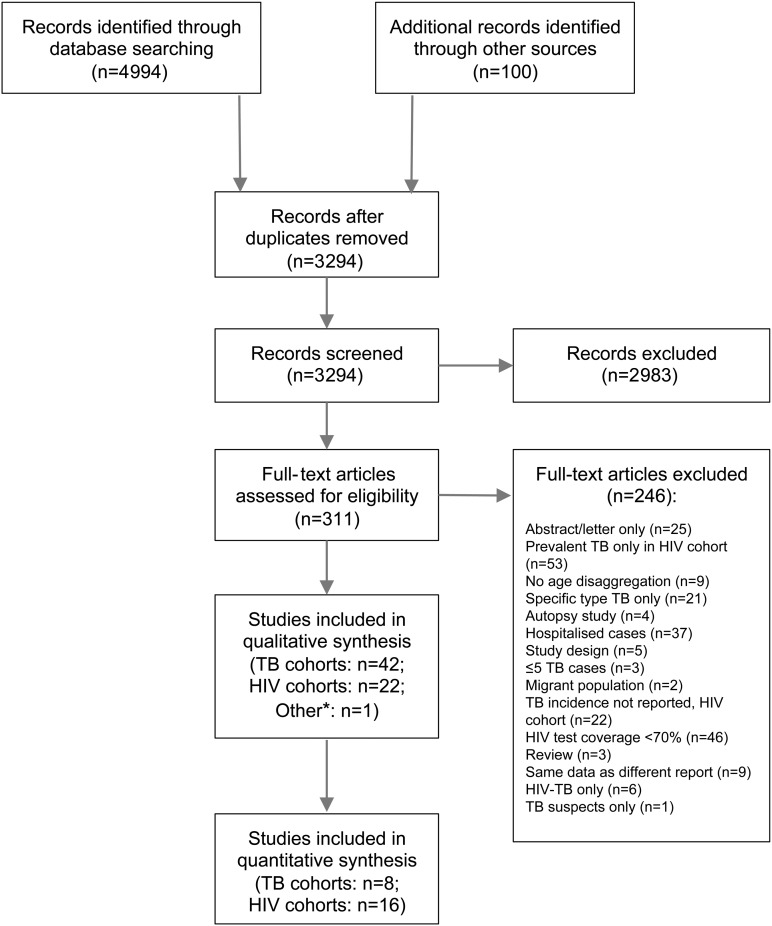
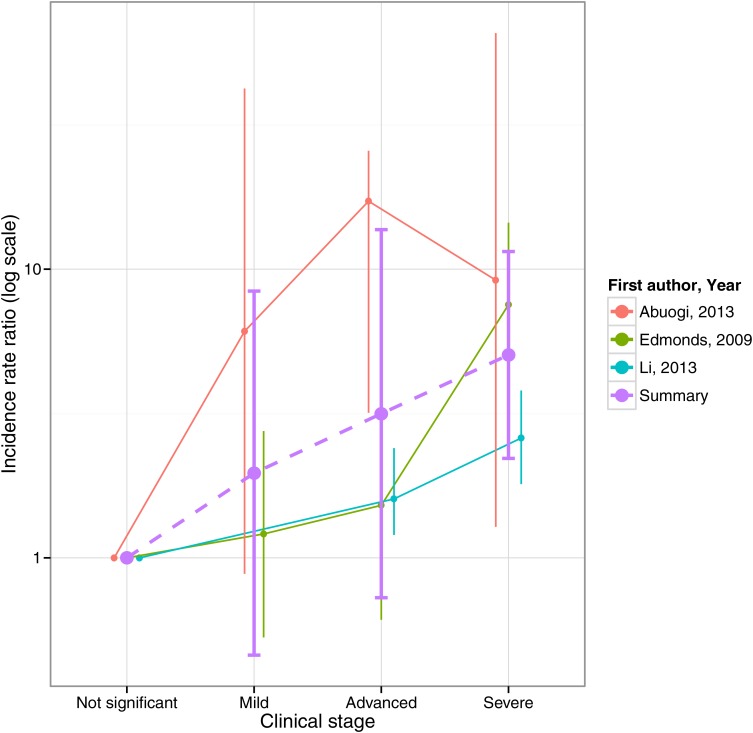
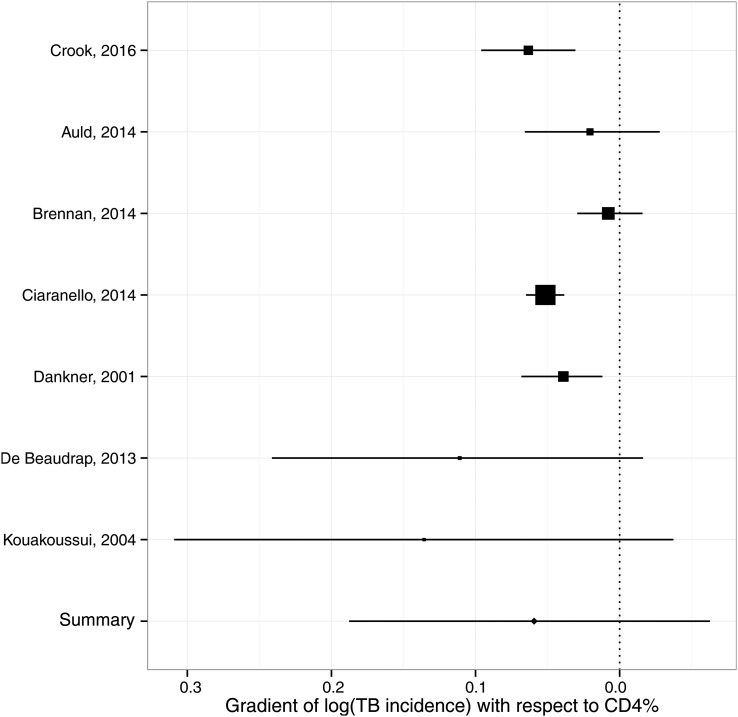
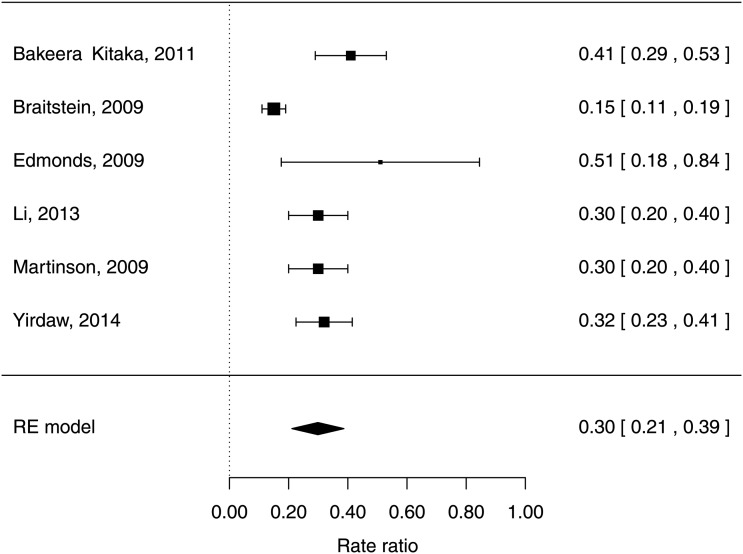
Methods: We searched MEDLINE and Embase for studies measuring HIV prevalence in paediatric TB cases ('TB cohorts') and paediatric HIV cohorts reporting TB incidence ('HIV cohorts'). Study quality was assessed using the Newcastle-Ottawa tool. TB cohorts with controls were meta-analysed to determine the incidence rate ratio (IRR) for TB given HIV. HIV cohort data were meta-analysed to estimate the trend in log-IRR versus CD4%, relative incidence by immunological stage and ART-associated protection from TB.
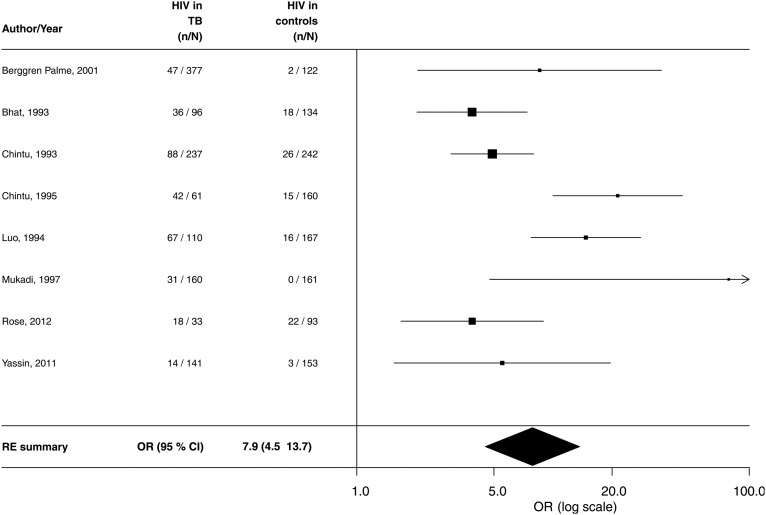
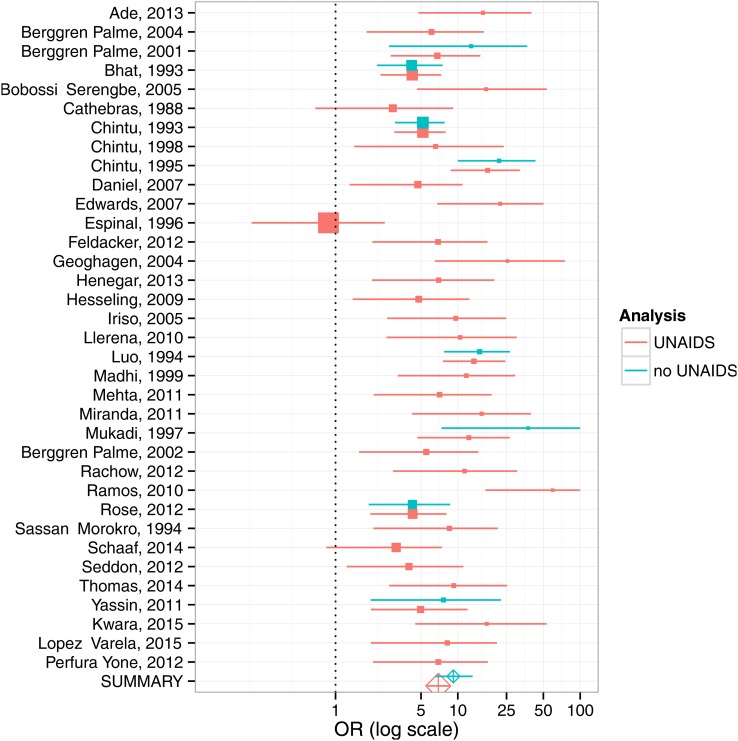
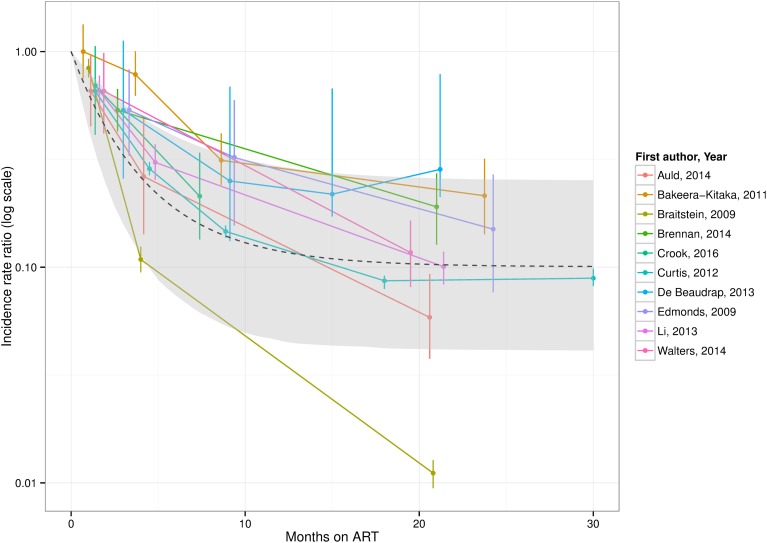
Results: 42 TB cohorts and 22 HIV cohorts were included. In the eight TB cohorts with controls, the IRR for TB was 7.9 (95% CI 4.5 to 13.7). HIV-infected children exhibited a reduction in IRR of 0.94 (95% credible interval: 0.83-1.07) per percentage point increase in CD4%. TB incidence was 5.0 (95% CI 4.0 to 6.0) times higher in children with severe compared with non-significant immunosuppression. TB incidence was lower in HIV-infected children on ART (HR: 0.30; 95% CI 0.21 to 0.39). Following initiation of ART, TB incidence declined rapidly over 12 months towards a HR of 0.10 (95% CI 0.04 to 0.25).
Conclusions: HIV is a potent risk factor for paediatric TB, and ART is strongly protective. In HIV-infected children, early diagnosis and ART initiation reduces TB risk.
Trial registration number: CRD42014014276.
Keywords: Tuberculosis.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Marais BJ, Gie RP, Schaaf HS, et al. The natural history of childhood intra-thoracic tuberculosis: a critical review of literature from the pre-chemotherapy era. Int J Tuberc Lung Dis 2004;8:392–402. - PubMed
-
- World Health Organization. Global tuberculosis report 2015. Geneva, 2015.
-
- UNAIDS. 2014 progress report on the global plan. Geneva, 2014.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials