

Implantation of a Poly-L-Lactide GCSF-Functionalized Scaffold in a Model of Chronic Myocardial Infarction
- PMID: 28116550
- PMCID: PMC5323505
- DOI: 10.1007/s12265-016-9718-9
Implantation of a Poly-L-Lactide GCSF-Functionalized Scaffold in a Model of Chronic Myocardial Infarction
Abstract
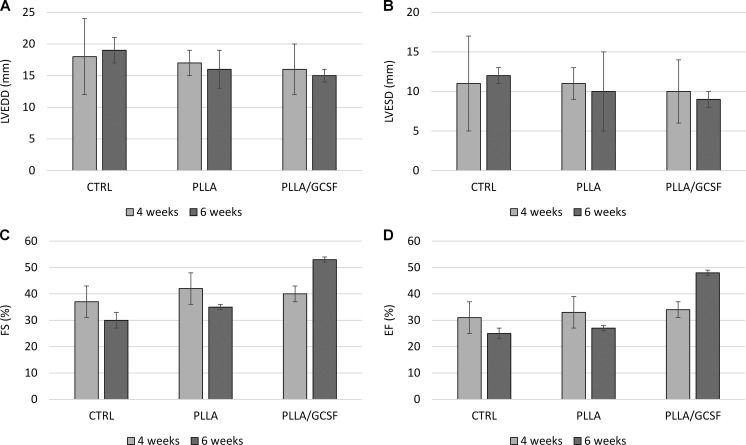
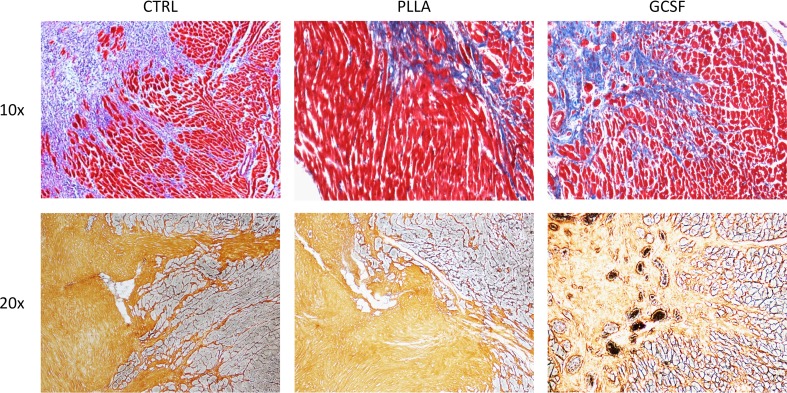
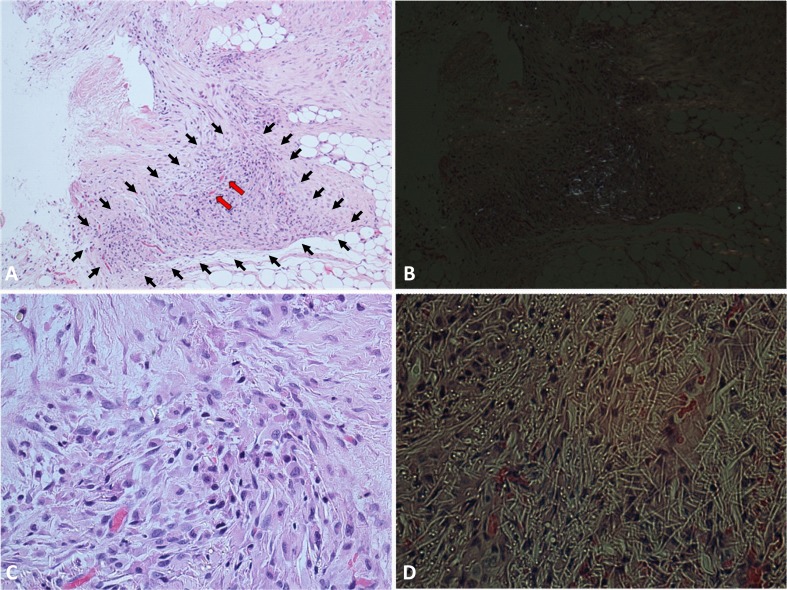
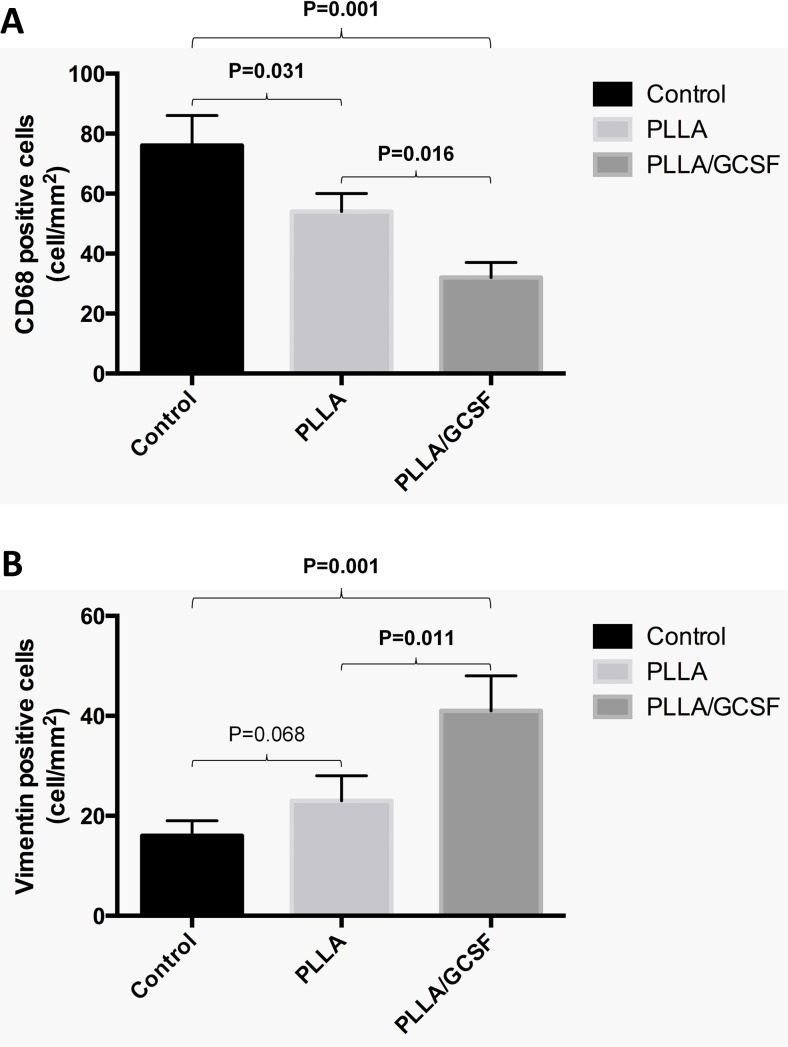
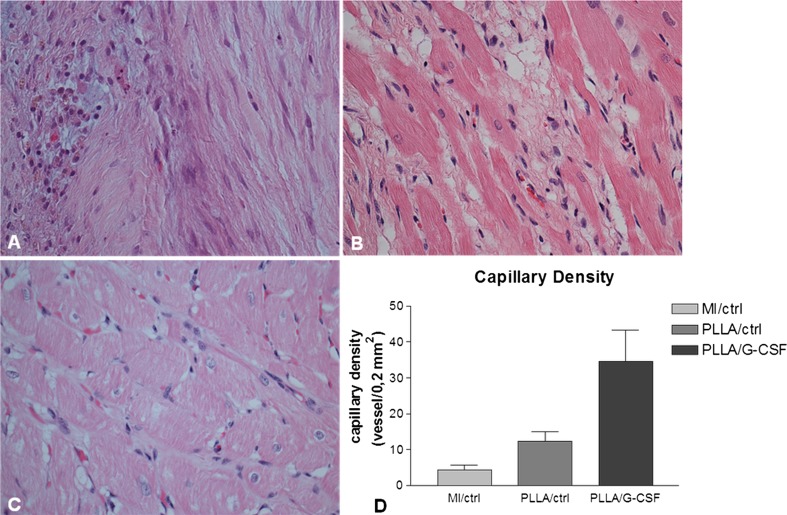
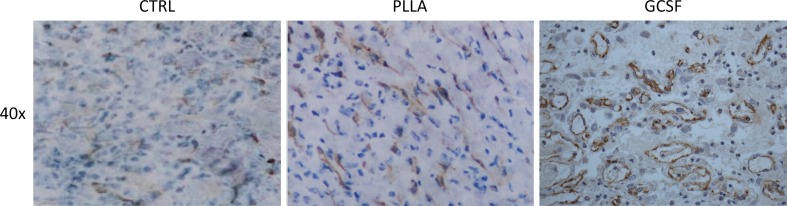
A previously developed poly-L-lactide scaffold releasing granulocyte colony-stimulating factor (PLLA/GCSF) was tested in a rabbit chronic model of myocardial infarction (MI) as a ventricular patch. Control groups were constituted by healthy, chronic MI and nonfunctionalized PLLA scaffold. PLLA-based electrospun scaffold efficiently integrated into a chronic infarcted myocardium. Functionalization of the biopolymer with GCSF led to increased fibroblast-like vimentin-positive cellular colonization and reduced inflammatory cell infiltration within the micrometric fiber mesh in comparison to nonfunctionalized scaffold; PLLA/GCSF polymer induced an angiogenetic process with a statistically significant increase in the number of neovessels compared to the nonfunctionalized scaffold; PLLA/GCSF implanted at the infarcted zone induced a reorganization of the ECM architecture leading to connective tissue deposition and scar remodeling. These findings were coupled with a reduction in end-systolic and end-diastolic volumes, indicating a preventive effect of the scaffold on ventricular dilation, and an improvement in cardiac performance.
Keywords: 3D scaffold; Cardiac graft; Electrospinning; GCSF; Myocardial infarction; PLLA; Tissue engineering.
Conflict of interest statement
Conflict of Interest
The authors declare that they have no conflict of interest.
Figures
References
-
- Frangogiannis NG. Chemokines in the ischemic myocardium: from inflammation to fibrosis. Inflammation Research. 2004;53(11):585–595. - PubMed
-
- Chamberlain DA. Overview of completed sudden death trials: European experience. Cardiology. 1987;74(Suppl 2):10–23. - PubMed
-
- Demirovic J, Myerburg RJ. Epidemiology of sudden coronary death: an overview. Progress in Cardiovascular Diseases. 1994;37(1):39–48. - PubMed
-
- Myerburg RJ, Kessler KM, Castellanos A. Sudden cardiac death. Structure, function, and time-dependence of risk. Circulation. 1992;85(1 Suppl):I2–10. - PubMed
-
- Kang, H. J., Kim, H. S., Koo, B. K., et al. (2007). Intracoronary infusion of the mobilized peripheral blood stem cell by G-CSF is better than mobilization alone by G-CSF for improvement of cardiac function and remodeling: 2-year follow-up results of the Myocardial Regeneration and Angiogenesis in Myocardial Infarction with G-CSF and Intra-Coronary Stem Cell Infusion (MAGIC Cell) 1 trial. Am Heart J, 153(2), 237 e231–238, doi:10.1016/j.ahj.2006.11.004. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
