

Is There an Association Between Hemoglobin A1C and Deep Postoperative Infection After TKA?
- PMID: 28116667
- PMCID: PMC5406337
- DOI: 10.1007/s11999-017-5246-4
Is There an Association Between Hemoglobin A1C and Deep Postoperative Infection After TKA?
Abstract
Background: Despite substantial research into the use of glycemic markers to stratify infection risk in patients with diabetes mellitus, there is little evidence to support a perioperative hemoglobin A1c (HbA1c) level associated with an increased risk of deep postoperative infection after TKA.
Questions/purposes: (1) Is there an association between perioperative HbA1c level in patients with diabetes and deep postoperative infection after primary TKA? (2) Is the perioperative HbA1c level in patients with diabetes a useful test as an independent predictor for postoperative infection after TKA?
Methods: We queried the PearlDiver Patient Records Database Humana dataset for patients who underwent primary TKA. This is a for-fee insurance patient-records database that contains records for more than 20 million patients with orthopaedic diagnoses from 2007 to the second quarter of 2015. The data for patients from this study were taken from the Humana dataset since this is the only insurer that includes laboratory data among the available databases. Although it is difficult to calculate attrition in this database, in the current study the minimum number of patients with at least 1 year followup was 86%. Patients with diabetes who had an HbA1c level obtained within 3 months of surgery were identified, stratified based on their HbA1c level in 0.5 mg/dL increments, and then compared with patients with diabetes without an HbA1c level within 3 months of surgery. Patients who had an HbA1c level within 3 months of surgery had slightly higher rates of polyneuropathy, chronic renal failure, and chronic kidney disease Stages 2 and 3. Otherwise, these groups were similar regarding rates of peripheral vascular disease, microvascular ischemic disease, metabolic syndrome, gastroparesis, end stage renal disease, age, and gender. Deep infection was defined as an infection resulting in operative intervention within 1 year of the primary TKA, and the incidence of such intervention for each HbA1c group then was identified. A receiver operating characteristic (ROC) analysis was performed to determine a threshold value of the HbA1c, and an area under the curve (AUC) analysis was performed to measure the accuracy and clinical utility of HbA1c as an independent predictor for postoperative infection.
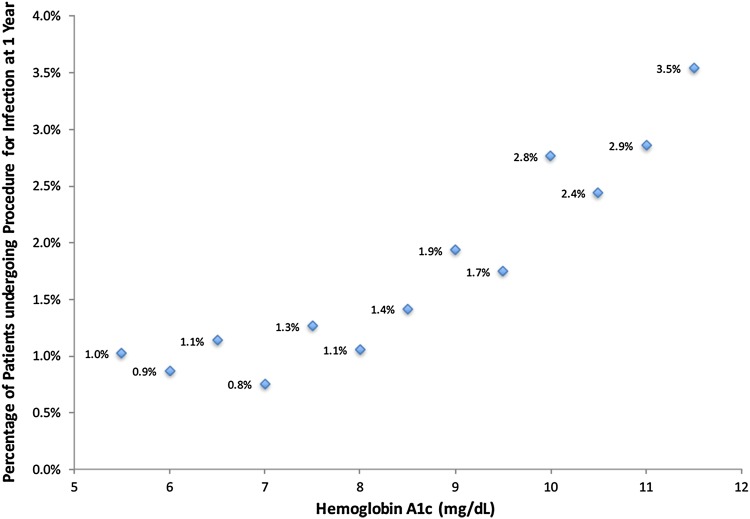
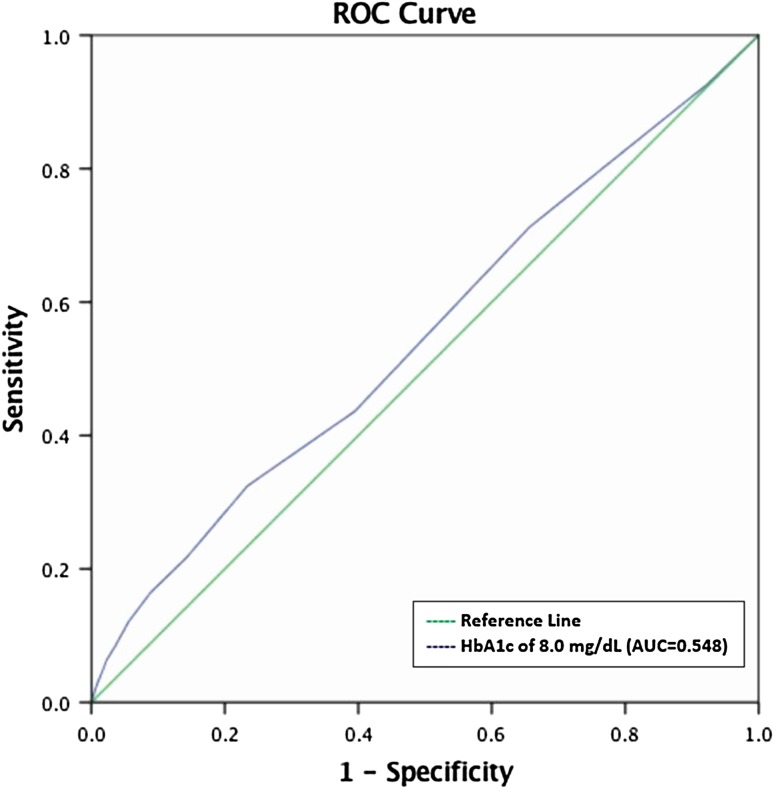
Results: The rate of infection requiring operative intervention ranged from a low of 0.8% with an HbA1c of 5.49 mg/dL or less, up to 3.5% for patients with HbA1c level greater than 11.5 mg/dL. The ROC analysis indicated that the best threshold was an HbA1c of 8.0 mg/dL (1.7; 95% CI, 1.2-2.4 mg/dL; p = 0.004), however, the AUC of 0.548 (95% CI, 0.50-0.59; p = 0.025) indicated that this threshold was inaccurate and only slightly better than chance, and thus alone could not serve as an independent discriminator of infection risk.
Conclusions: The risk of deep postoperative infection requiring surgical intervention after TKA in patients with diabetes mellitus increases as the perioperative HbA1c increases. While a threshold HbA1c level of 8.0 mg/dL was identified, it cannot by itself serve as an independent predictor of postoperative infection in patients with diabetes mellitus because its sensitivity is so low. Future studies should determine what other confounders other than an elevated HbA1c level contribute to increased infection risk and whether decreasing HbA1c levels before TKA will decrease the subsequent risk of infection after surgery.
Level of evidence: Level III, diagnostic study.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
