

IL-22-producing CD4+T cells in the treatment response of rheumatoid arthritis to combination therapy with methotrexate and leflunomide
- PMID: 28117352
- PMCID: PMC5259708
- DOI: 10.1038/srep41143
IL-22-producing CD4+T cells in the treatment response of rheumatoid arthritis to combination therapy with methotrexate and leflunomide
Abstract
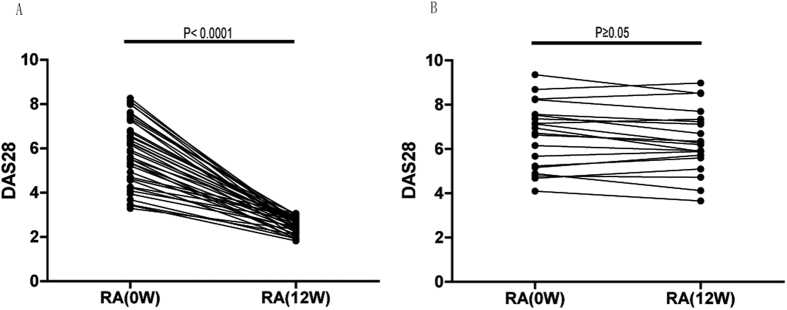
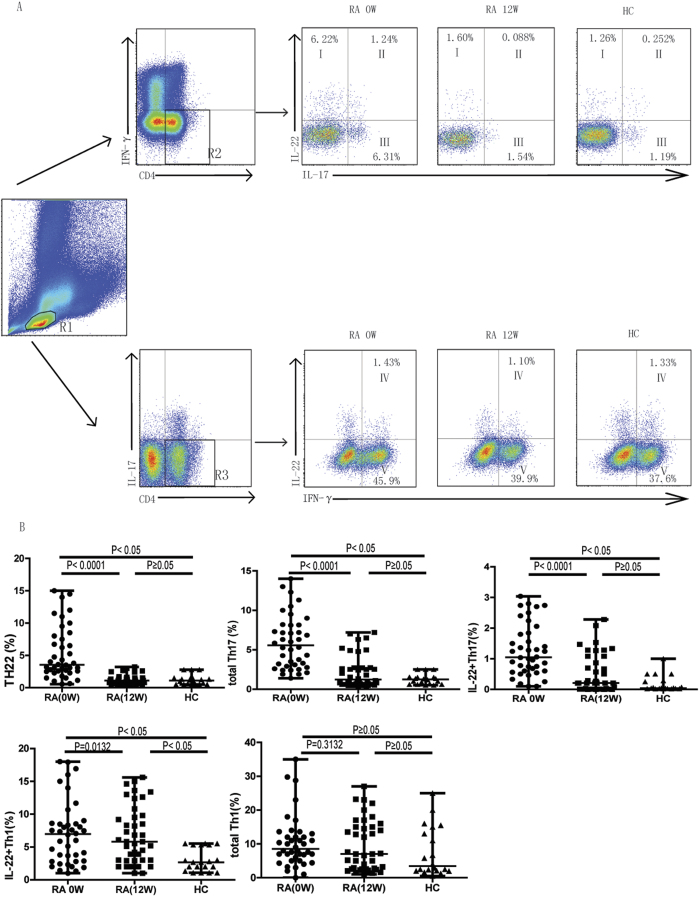
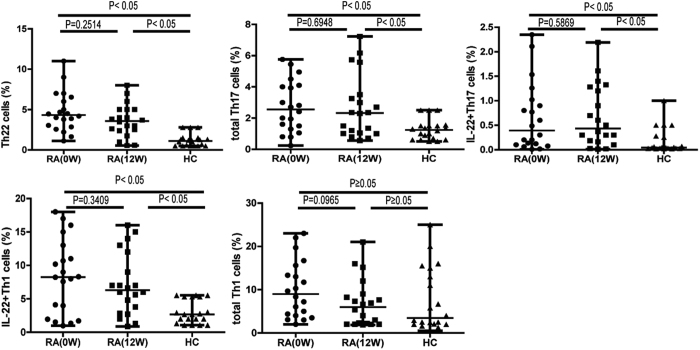
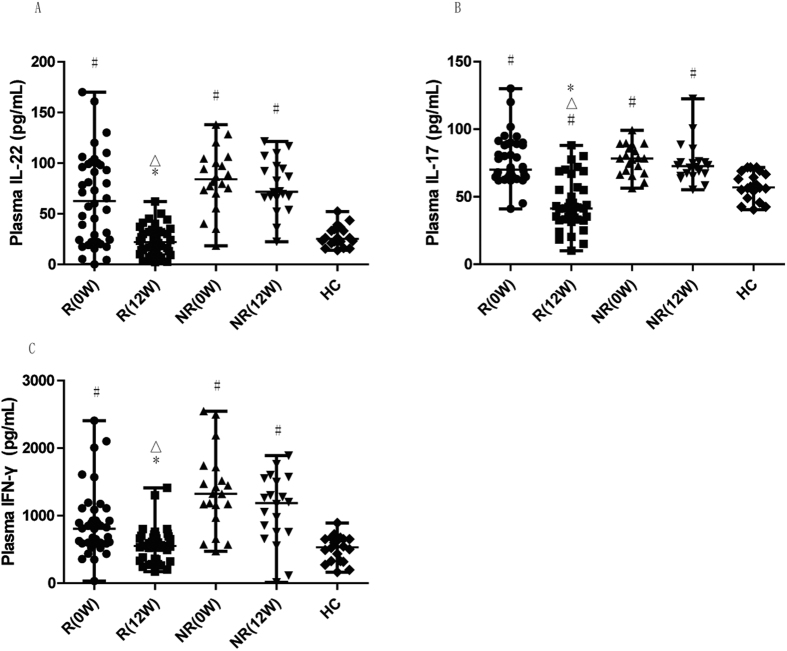
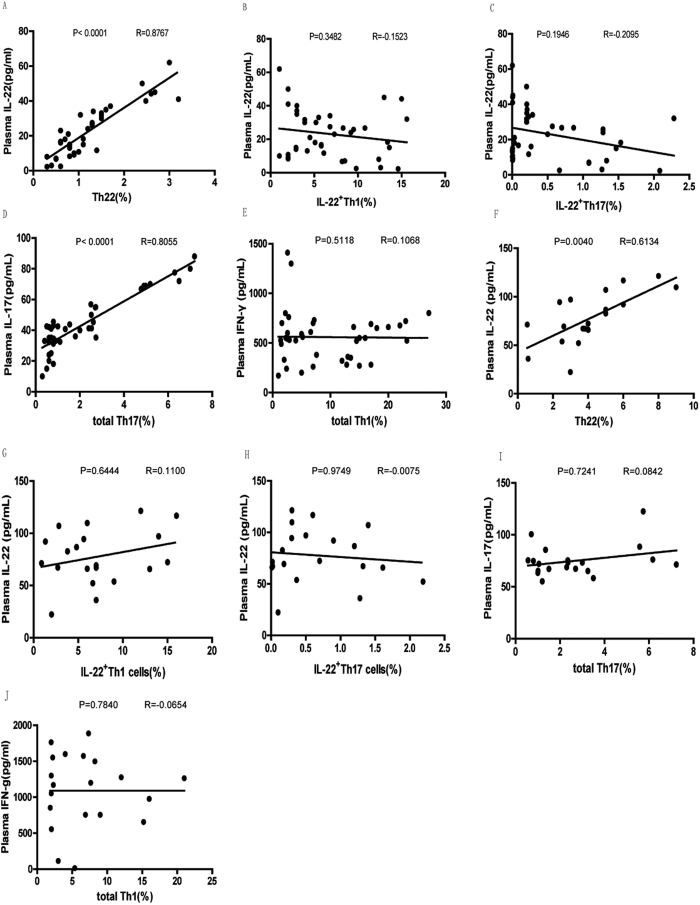
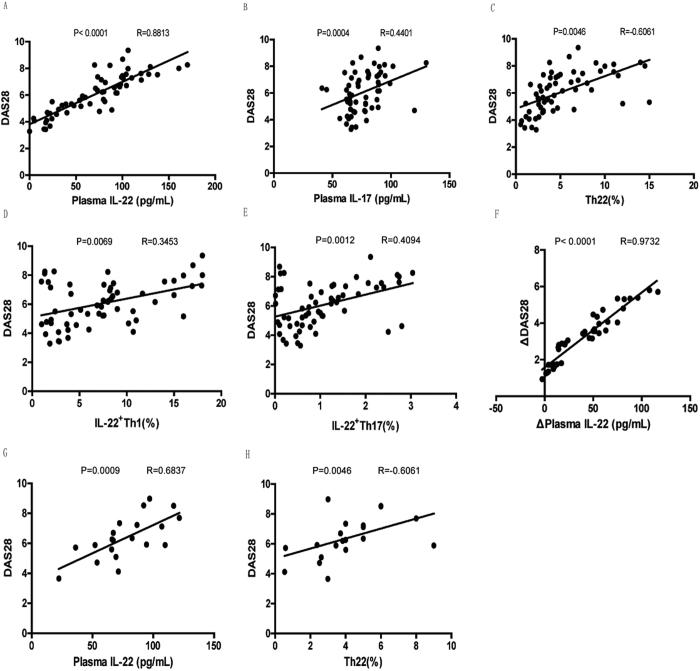
T cells are key players in immune-mediated rheumatoid arthritis (RA). We previously reported that interleukin (IL)-22+CD4+T helper (IL-22+ Th) cells and IL-22 critically control the pathogenesis of RA. Here we monitored circulating levels of different IL-22+ Th cell subsets and measured plasma levels of IL-22, IL-17, and interferon (IFN)-γ in 60 patients with active RA following 12-week combination methotrexate (MTX) and leflunomide (LEF) therapy (MTX+LEF) and 20 healthy individuals. We found the frequencies of circulating IFN-γ-IL-17-IL-22+ (Th22), IFN-γ-IL-17+ (total Th17), IFN-γ+IL-17-IL-22+ (IL-22+Th1) cells, and IFN-γ-IL-17+IL-22+ (IL-22+Th17) cells, as well as the plasma levels of IL-22, IL-17 and IFN-γ to be significantly reduced in RA patients that responded to treatment, but not in non-responders. Reductions in plasma IL-22 level significantly correlated with percentage of circulating Th22 cells and the decrease of plasma IL-22 level correlated with the reduction of DAS28 in responders. Our data suggests that circulating Th22 cells and plasma IL-22 level play a detrimental role in RA. The combination MTX+LEF therapy, by targeting Th22 cells and reducing IL-22 level, relieves the immune defects and ameliorates symptoms of RA. This study provides novel mechanistic understanding of the pathogenesis of RA, which may promote a design of better therapies for RA.
Conflict of interest statement
The authors declare that they have no competing financial interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
