

Utilization of biopsy-based genomic classifier to predict distant metastasis after definitive radiation and short-course ADT for intermediate and high-risk prostate cancer
- PMID: 28117383
- PMCID: PMC5435968
- DOI: 10.1038/pcan.2016.58
Utilization of biopsy-based genomic classifier to predict distant metastasis after definitive radiation and short-course ADT for intermediate and high-risk prostate cancer
Abstract
Background: We examined the ability of a biopsy-based 22-marker genomic classifier (GC) to predict for distant metastases after radiation and a median of 6 months of androgen deprivation therapy (ADT).
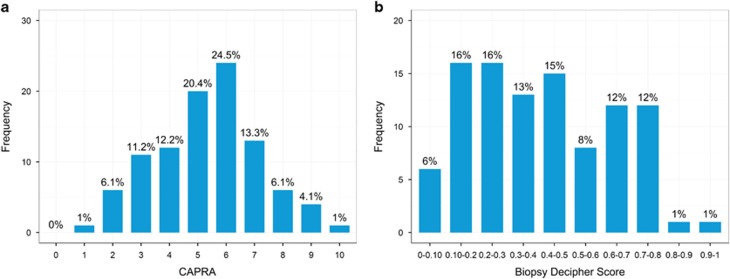
Methods: We studied 100 patients with intermediate-risk (55%) and high-risk (45%) prostate cancer who received definitive radiation plus a median of 6 months of ADT (range 3-39 months) from 2001-2013 at a single center and had available biopsy tissue. Six to ten 4 micron sections of the needle biopsy core with the highest Gleason score and percentage of tumor involvement were macrodissected for RNA extraction. GC scores (range, 0.04-0.92) were determined. The primary end point of the study was time to distant metastasis. Median follow-up was 5.1 years. There were 18 metastases during the study period.
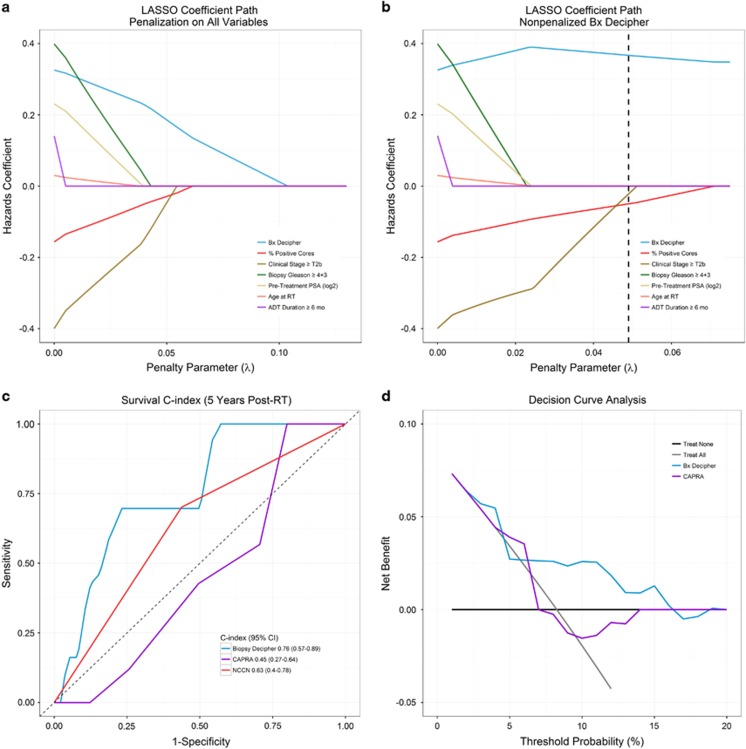
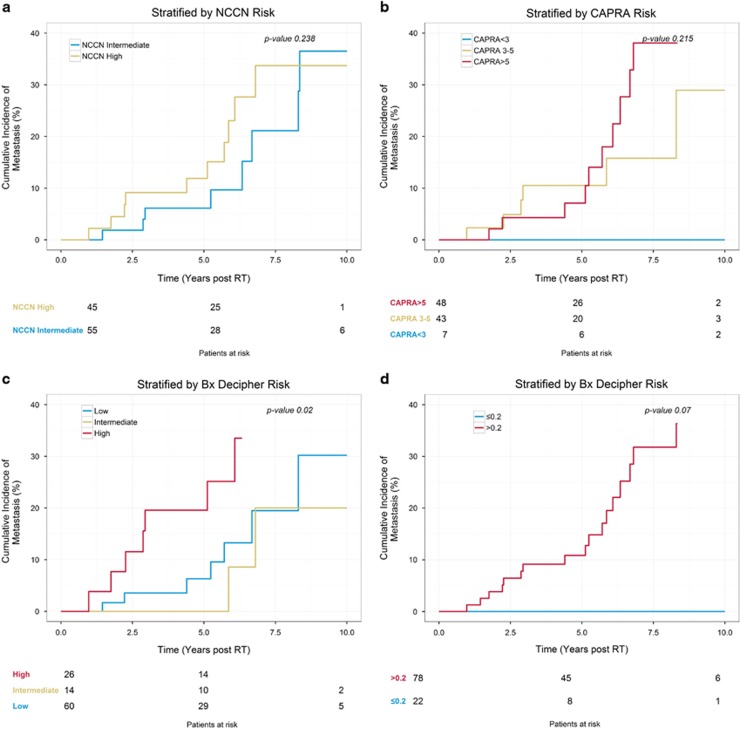
Results: On univariable analysis (UVA), each 0.1 unit increase in GC score was significantly associated with time to distant metastasis (hazard ratio: 1.40 (1.10-1.84), P=0.006) and remained significant after adjusting for clinical variables on multivariable analysis (MVA) (adjusted hazard ratio: 1.36 (1.04-1.83), P=0.024). The c-index for 5-year distant metastasis was 0.45 (95% confidence interval: 0.27-0.64) for Cancer of the Prostate Risk Assessment score, 0.63 (0.40-0.78) for National Comprehensive Cancer Network (NCCN) risk groups, and 0.76 (0.57-0.89) for the GC score. Using pre-specified GC risk categories, the cumulative incidence of metastasis for GC>0.6 reached 20% at 5 years after radiation (P=0.02).
Conclusions: We believe this is the first demonstration of the ability of the biopsy-based GC score to predict for distant metastases after definitive radiation and ADT for intermediate- and high-risk prostate cancer. Patients with the highest GC risk (GC>0.6) had high rates of metastasis despite multi-modal therapy suggesting that they could potentially be candidates for treatment intensification and/or enrollment in clinical trials of novel therapy.
Conflict of interest statement
PLN has consulted for Medivation, GenomeDx and Ferring. FYF has consulted for Medivation and GenomeDx. NEM has received personal fees from Via Oncology. VC, BP-A, TK, HS and ED are all employees of GenomeDx Biosciences. The remaining authors declare no conflicts of interest.
Figures
References
-
- Mohler JL, Armstrong AJ, Bahnson RR, D'Amico AV, Davis BJ, Eastham JA et al. Prostate cancer, version 1. 2016. J Natl Compr Canc Netw 2016; 14: 19–30. - PubMed
-
- Klein EA, Cooperberg MR, Magi-Galluzzi C, Simko JP, Falzarano SM, Maddala T et al. A 17-gene assay to predict prostate cancer aggressiveness in the context of Gleason grade heterogeneity, tumor multifocality, and biopsy undersampling. Eur Urol 2014; 66: 550–560. - PubMed
-
- Klein EA, Haddad Z, Yousefi K, Lam LLC, Wang Q, Choeurng V et al. Decipher genomic classifier measured on prostate biopsy predicts metastasis risk. Urology 2016; 90: 148–152. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
